

Using Mobile Virtual Reality Simulation to Prepare for In-Person Helping Babies Breathe Training: Secondary Analysis of a Randomized Controlled Trial (the eHBB/mHBS Trial)
- PMID: 36094807
- PMCID: PMC9513689
- DOI: 10.2196/37297
Using Mobile Virtual Reality Simulation to Prepare for In-Person Helping Babies Breathe Training: Secondary Analysis of a Randomized Controlled Trial (the eHBB/mHBS Trial)
Abstract
Background: Neonatal mortality accounts for approximately 46% of global under-5 child mortality. The widespread access to mobile devices in low- and middle-income countries has enabled innovations, such as mobile virtual reality (VR), to be leveraged in simulation education for health care workers.
Objective: This study explores the feasibility and educational efficacy of using mobile VR for the precourse preparation of health care professionals in neonatal resuscitation training.
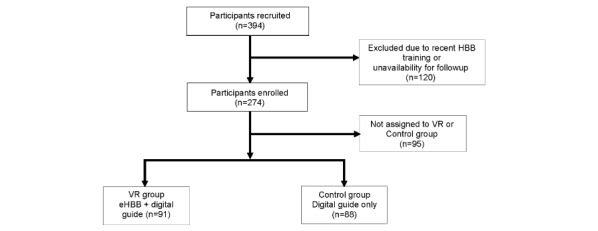
Methods: Health care professionals in obstetrics and newborn care units at 20 secondary and tertiary health care facilities in Lagos, Nigeria, and Busia, Western Kenya, who had not received training in Helping Babies Breathe (HBB) within the past 1 year were randomized to access the electronic HBB VR simulation and digitized HBB Provider's Guide (VR group) or the digitized HBB Provider's Guide only (control group). A sample size of 91 participants per group was calculated based on the main study protocol that was previously published. Participants were directed to use the electronic HBB VR simulation and digitized HBB Provider's Guide or the digitized HBB Provider's Guide alone for a minimum of 20 minutes. HBB knowledge and skills assessments were then conducted, which were immediately followed by a standard, in-person HBB training course that was led by study staff and used standard HBB evaluation tools and the Neonatalie Live manikin (Laerdal Medical).
Results: A total of 179 nurses and midwives participated (VR group: n=91; control group: n=88). The overall performance scores on the knowledge check (P=.29), bag and mask ventilation skills check (P=.34), and Objective Structured Clinical Examination A checklist (P=.43) were similar between groups, with low overall pass rates (6/178, 3.4% of participants). During the Objective Structured Clinical Examination A test, participants in the VR group performed better on the critical step of positioning the head and clearing the airway (VR group: 77/90, 86%; control group: 57/88, 65%; P=.002). The median percentage of ventilations that were performed via head tilt, as recorded by the Neonatalie Live manikin, was also numerically higher in the VR group (75%, IQR 9%-98%) than in the control group (62%, IQR 13%-97%), though not statistically significantly different (P=.35). Participants in the control group performed better on the identifying a helper and reviewing the emergency plan step (VR group: 7/90, 8%; control group: 16/88, 18%; P=.045) and the washing hands step (VR group: 20/90, 22%; control group: 32/88, 36%; P=.048).
Conclusions: The use of digital interventions, such as mobile VR simulations, may be a viable approach to precourse preparation in neonatal resuscitation training for health care professionals in low- and middle-income countries.
Keywords: Helping Babies Breathe; digital education; digital intervention; health care education; health care worker; medical education; mobile Helping Babies Survive powered by District Health Information Software 2; mobile learning; neonatal mortality; neonatal resuscitation; virtual reality.
©Beatrice Nkolika Ezenwa, Rachel Umoren, Iretiola Bamikeolu Fajolu, Daniel S Hippe, Sherri Bucher, Saptarshi Purkayastha, Felicitas Okwako, Fabian Esamai, John B Feltner, Olubukola Olawuyi, Annet Mmboga, Mary Concepta Nafula, Chris Paton, Veronica Chinyere Ezeaka. Originally published in JMIR Medical Education (https://mededu.jmir.org), 12.09.2022.
Conflict of interest statement
Conflicts of Interest: RU and CP developed the eHBB VR app. SB and SP developed the mHBS/DHIS2 app. All other coauthors have no conflicts of interest to disclose that are relevant to this article.
Figures
References
-
- Perin J, Mulick A, Yeung D, Villavicencio F, Lopez G, Strong KL, Prieto-Merino D, Cousens S, Black RE, Liu L. Global, regional, and national causes of under-5 mortality in 2000-19: an updated systematic analysis with implications for the Sustainable Development Goals. Lancet Child Adolesc Health. 2022 Feb;6(2):106–115. doi: 10.1016/S2352-4642(21)00311-4. https://linkinghub.elsevier.com/retrieve/pii/S2352-4642(21)00311-4 S2352-4642(21)00311-4 - DOI - PMC - PubMed
-
- Pammi M, Dempsey EM, Ryan CA, Barrington KJ. Newborn resuscitation training programmes reduce early neonatal mortality. Neonatology. 2016;110(3):210–224. doi: 10.1159/000443875. https://www.karger.com?DOI=10.1159/000443875 000443875 - DOI - PubMed
-
- Matendo R, Engmann C, Ditekemena J, Gado J, Tshefu A, Kinoshita R, McClure EM, Moore J, Wallace D, Carlo WA, Wright LL, Bose C. Reduced perinatal mortality following enhanced training of birth attendants in the Democratic Republic of Congo: a time-dependent effect. BMC Med. 2011 Aug 04;9:93. doi: 10.1186/1741-7015-9-93. https://bmcmedicine.biomedcentral.com/articles/10.1186/1741-7015-9-93 1741-7015-9-93 - DOI - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
