

Use of common blood parameters for the differential diagnosis of childhood infections
- PMID: 36095013
- PMCID: PMC9467365
- DOI: 10.1371/journal.pone.0273236
Use of common blood parameters for the differential diagnosis of childhood infections
Abstract
Background: Routine laboratory investigations are not rapidly available to assist clinicians in the diagnosis of pediatric acute infections. Our objective was to evaluate some common blood parameters and use them for the differential diagnosis of childhood infections.
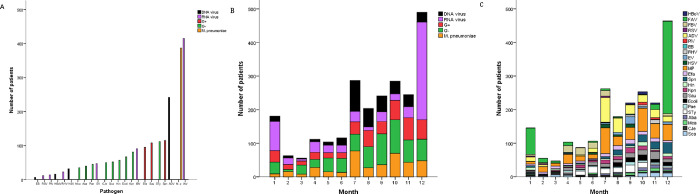
Methods: This retrospective study was conducted between October 2019 and September 2020 at Guangzhou Women and Children's Medical Center, China. We performed blood tests in patients infected with DNA viruses (n = 402), RNA viruses (n = 602), gram-positive organisms (G+; n = 421), gram-negative organisms (G-; n = 613), or Mycoplasma pneumoniae (n = 387), as well as in children without infection (n = 277). The diagnostic utility of blood parameters to diagnose various infections was evaluated by logistic regression analysis.
Results: The most common G+ organism, G- organism, and virus were Streptococcus pneumoniae (39.7%), Salmonella typhimurium (18.9%), and influenza A virus (40.2%), respectively. The value of logit (P) = 0.003 × C-reactive protein (CRP) - 0.011 × hemoglobin (HGB) + 0.001 × platelets (PLT) was significantly different between the control, RNA virus, DNA virus, M. pneumoniae, G- organism, and G+ organism groups (2.46 [95% CI, 2.41-2.52], 2.60 [2.58-2.62], 2.70 [2.67-2.72], 2.78 [2.76-2.81], 2.88 [2.85-2.91], and 2.97 [2.93-3.00], respectively; p = 0.00 for all). The logistic regression-based model showed significantly greater accuracy than the best single discriminatory marker for each group (logit [Pinfection] vs. CRP, 0.90 vs. 0.84, respectively; logit [PRNA] vs. lymphocytes, 0.83 vs. 0.77, respectively; p = 0.00). The area under curve values were 0.72 (0.70-0.74) for HGB and 0.81 (0.79-0.82) for logit (Pvirus/bacteria) to diagnose bacterial infections, whereas they were 0.72 (0.68-0.74) for eosinophils and 0.80 (0.78-0.82) for logit (Pvirus/bacteria) to diagnose viral infections. Logit (Pvirus/bacteria) < -0.45 discriminated bacterial from viral infection with 78.9% specificity and 70.7% sensitivity.
Conclusions: The combination of CRP, HGB, PLT, eosinophil, monocyte, and lymphocyte counts can distinguish between the infectious pathogens in children.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


References
-
- Andreeva E and Melbye H. Usefulness of C-reactive protein testing in acute cough/respiratory tract infection: an open cluster-randomized clinical trial with C-reactive protein testing in the intervention group. Bmc Fam Pract 2014; 15: 80. Journal Article; Randomized Controlled Trial. doi: 10.1186/1471-2296-15-80 - DOI - PMC - PubMed
-
- Yu Z, Jing H and Hongtao P, et al. Distinction between bacterial and viral infections by serum measurement of human neutrophil lipocalin (HNL) and the impact of antibody selection. J. Immunol. Methods 2016; 432: 82–86. Comparative Study; Journal Article. doi: 10.1016/j.jim.2016.02.014 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
