

Disentangling self from pain: mindfulness meditation-induced pain relief is driven by thalamic-default mode network decoupling
- PMID: 36095039
- PMCID: PMC9823141
- DOI: 10.1097/j.pain.0000000000002731
Disentangling self from pain: mindfulness meditation-induced pain relief is driven by thalamic-default mode network decoupling
Abstract
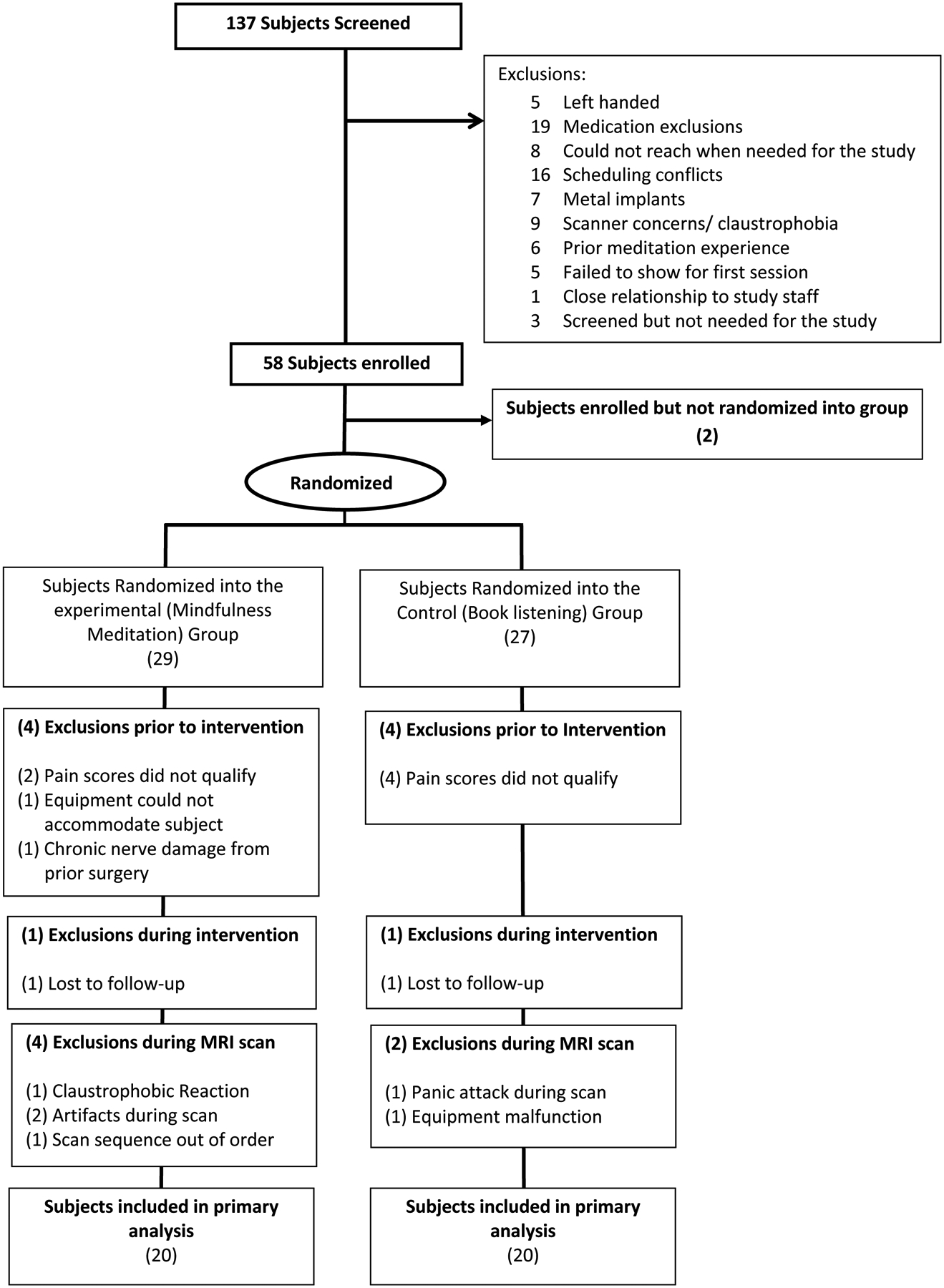
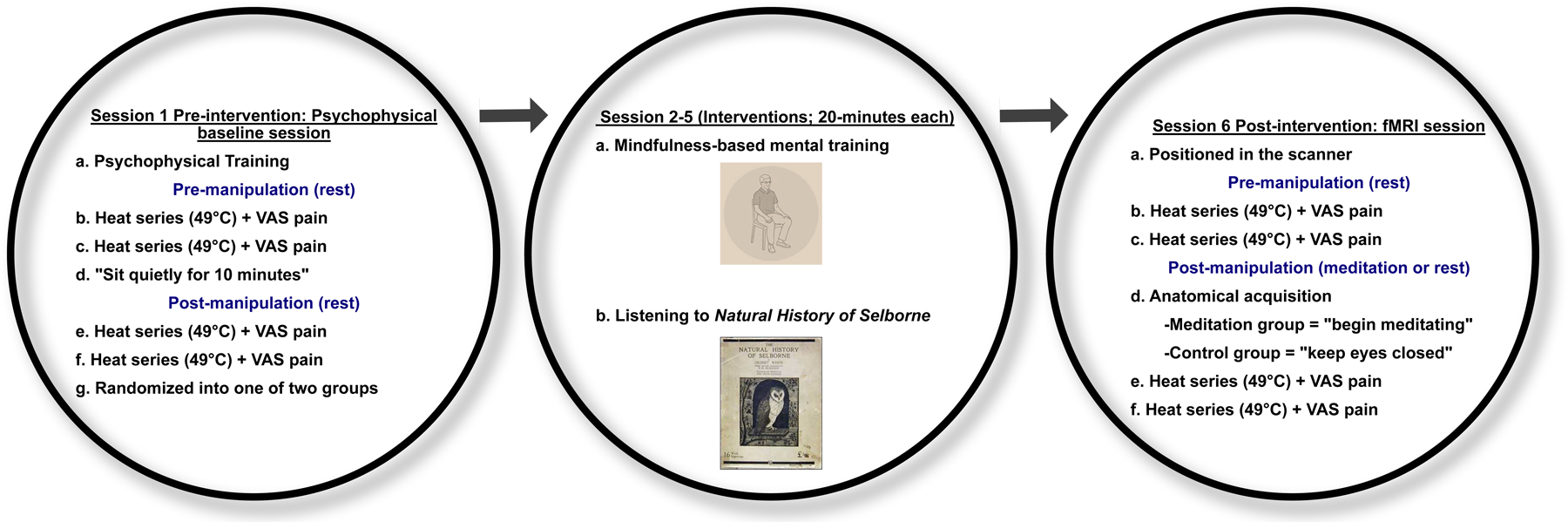
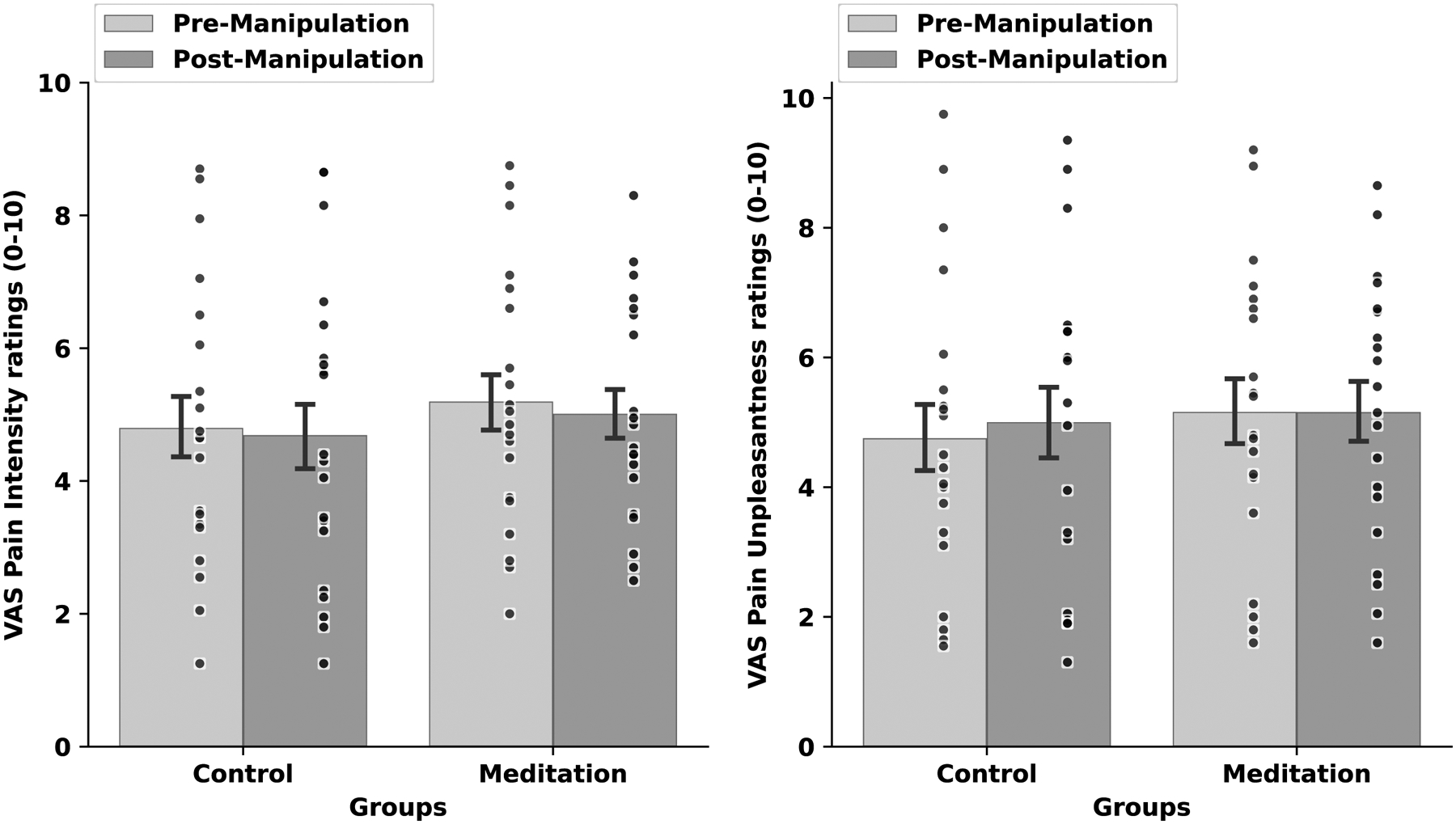
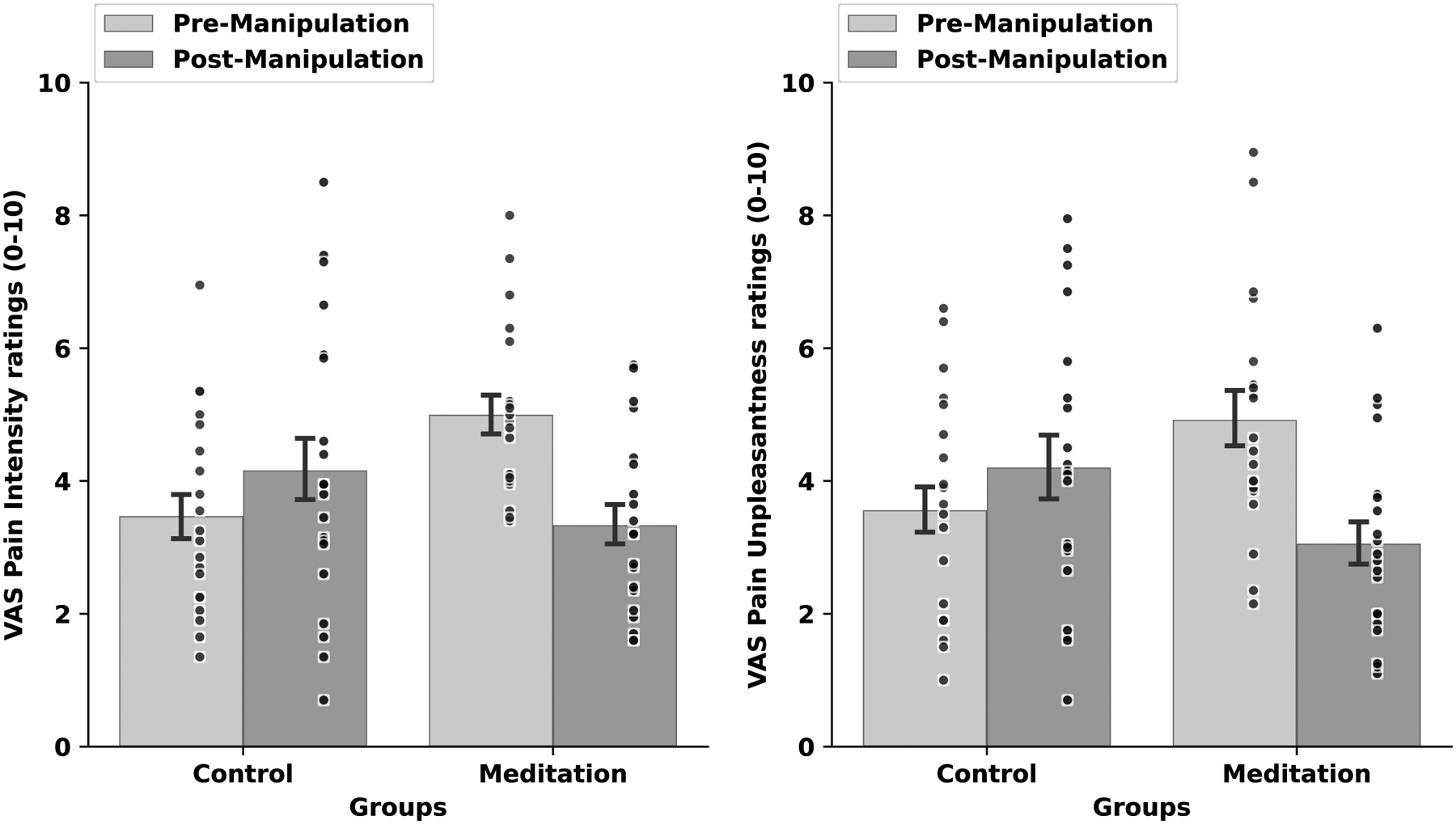
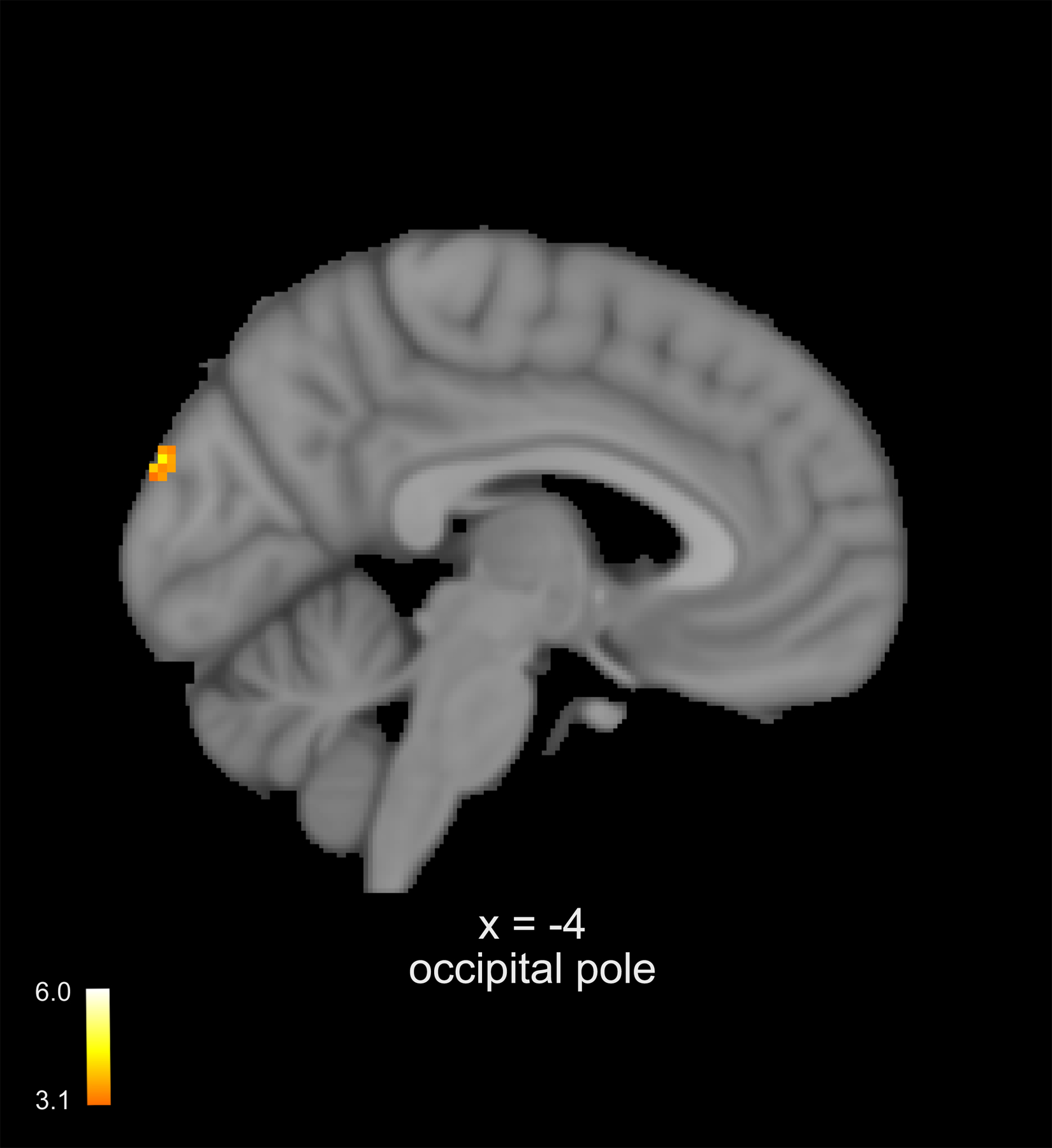
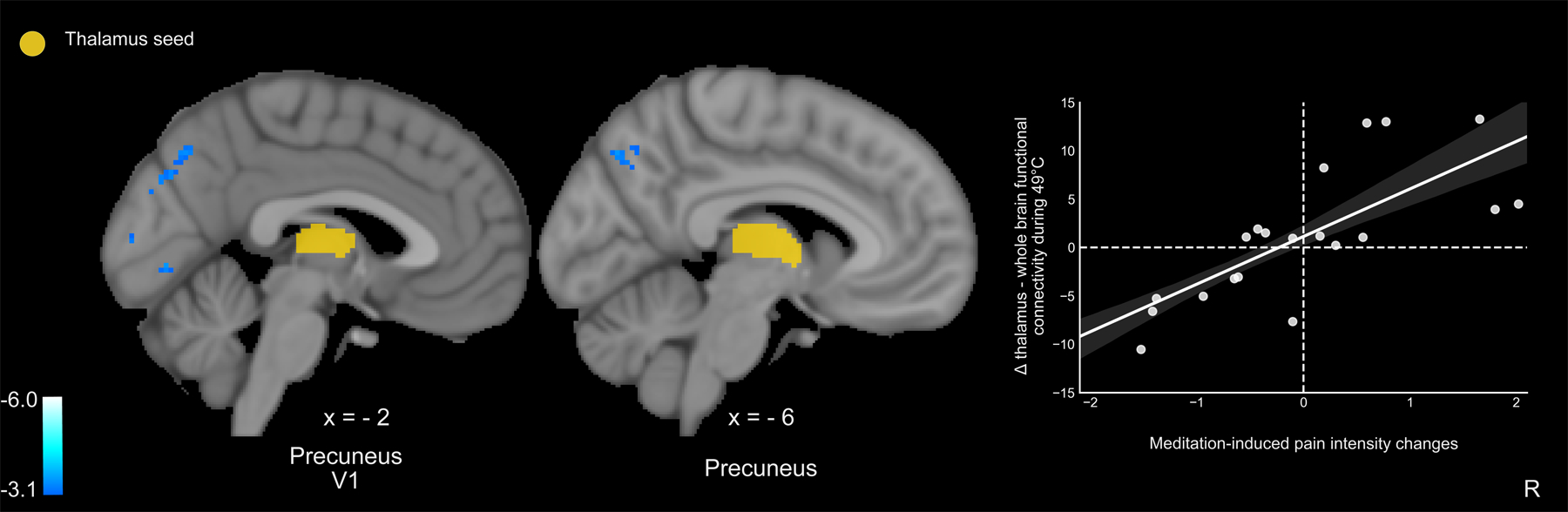
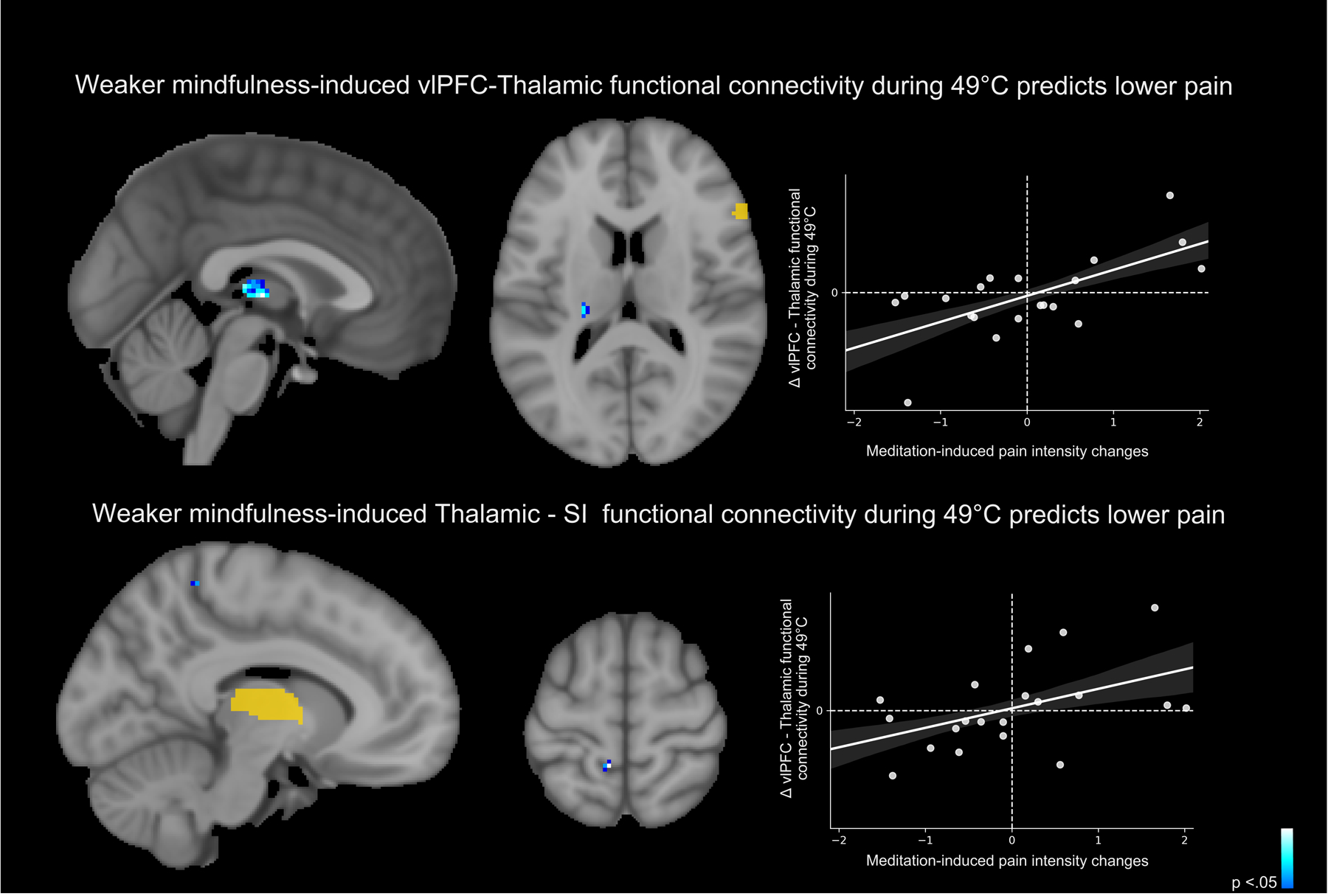
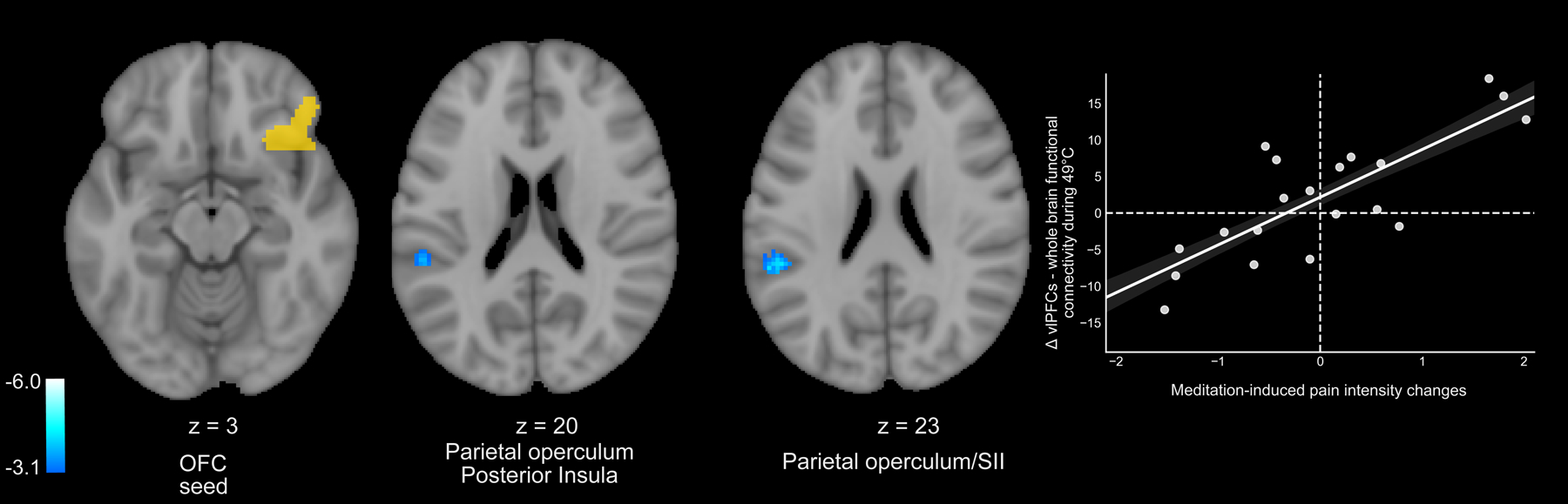
For millenniums, mindfulness was believed to diminish pain by reducing the influence of self-appraisals of noxious sensations. Today, mindfulness meditation is a highly popular and effective pain therapy that is believed to engage multiple, nonplacebo-related mechanisms to attenuate pain. Recent evidence suggests that mindfulness meditation-induced pain relief is associated with the engagement of unique cortico-thalamo-cortical nociceptive filtering mechanisms. However, the functional neural connections supporting mindfulness meditation-based analgesia remain unknown. This mechanistically focused clinical trial combined functional magnetic resonance imaging with psychophysical pain testing (49°C stimulation and pain visual analogue scales) to identify the neural connectivity supporting the direct modulation of pain-related behavioral and neural responses by mindfulness meditation. We hypothesized that mindfulness meditation-based pain relief would be reflected by greater decoupling between brain mechanisms supporting appraisal (prefrontal) and nociceptive processing (thalamus). After baseline pain testing, 40 participants were randomized to a well-validated, 4-session mindfulness meditation or book-listening regimen. Functional magnetic resonance imaging and noxious heat (49°C; right calf) were combined during meditation to test study hypotheses. Mindfulness meditation significantly reduced behavioral and neural pain responses when compared to the controls. Preregistered (NCT03414138) whole-brain analyses revealed that mindfulness meditation-induced analgesia was moderated by greater thalamus-precuneus decoupling and ventromedial prefrontal deactivation, respectively, signifying a pain modulatory role across functionally distinct neural mechanisms supporting self-referential processing. Two separate preregistered seed-to-seed analyses found that mindfulness meditation-based pain relief was also associated with weaker contralateral thalamic connectivity with the prefrontal and primary somatosensory cortex, respectively. Thus, we propose that mindfulness meditation is associated with a novel self-referential nociceptive gating mechanism to reduce pain.
Copyright © 2022 International Association for the Study of Pain.
Conflict of interest statement
DECLARATION OF INTERESTS
The authors declare no competing interests.
Figures

Similar articles
-
Mindfulness Meditation-Based Pain Relief Employs Different Neural Mechanisms Than Placebo and Sham Mindfulness Meditation-Induced Analgesia.J Neurosci. 2015 Nov 18;35(46):15307-25. doi: 10.1523/JNEUROSCI.2542-15.2015. J Neurosci. 2015. PMID: 26586819 Free PMC article. Clinical Trial.
-
Mindfulness Meditation and Placebo Modulate Distinct Multivariate Neural Signatures to Reduce Pain.Biol Psychiatry. 2025 Jan 1;97(1):81-88. doi: 10.1016/j.biopsych.2024.08.023. Epub 2024 Aug 30. Biol Psychiatry. 2025. PMID: 39216636 Clinical Trial.
-
The neural mechanisms of mindfulness-based pain relief: a functional magnetic resonance imaging-based review and primer.Pain Rep. 2019 Aug 7;4(4):e759. doi: 10.1097/PR9.0000000000000759. eCollection 2019 Jul-Aug. Pain Rep. 2019. PMID: 31579851 Free PMC article. Review.
-
The Role of Heart Rate Variability in Mindfulness-Based Pain Relief.J Pain. 2020 Mar-Apr;21(3-4):306-323. doi: 10.1016/j.jpain.2019.07.003. Epub 2019 Aug 1. J Pain. 2020. PMID: 31377215 Free PMC article. Clinical Trial.
-
Neurophysiological Mechanisms Supporting Mindfulness Meditation-Based Pain Relief: an Updated Review.Curr Pain Headache Rep. 2020 Aug 17;24(10):56. doi: 10.1007/s11916-020-00890-8. Curr Pain Headache Rep. 2020. PMID: 32803491 Review.
Cited by
-
Impact of Spinal Manipulative Therapy on Brain Function and Pain Alleviation in Lumbar Disc Herniation: A Resting-State fMRI Study.Chin J Integr Med. 2025 Feb;31(2):108-117. doi: 10.1007/s11655-024-4205-7. Epub 2024 Dec 21. Chin J Integr Med. 2025. PMID: 39707137
-
An update on non-pharmacological interventions for pain relief.Cell Rep Med. 2025 Feb 18;6(2):101940. doi: 10.1016/j.xcrm.2025.101940. Cell Rep Med. 2025. PMID: 39970872 Free PMC article. Review.
-
Thalamocortical Mechanisms Underlying Real and Imagined Acupuncture.Biomedicines. 2023 Jun 26;11(7):1830. doi: 10.3390/biomedicines11071830. Biomedicines. 2023. PMID: 37509469 Free PMC article.
-
The Mindful Reappraisal of Pain Scale (MRPS): Validation of a New Measure of Psychological Mechanisms of Mindfulness-Based Analgesia.Mindfulness (N Y). 2023 Jan;14(1):192-204. doi: 10.1007/s12671-022-02034-y. Epub 2022 Dec 16. Mindfulness (N Y). 2023. PMID: 37901118 Free PMC article.
-
Relationships between Self-Talk, Inner Speech, Mind Wandering, Mindfulness, Self-Concept Clarity, and Self-Regulation in University Students.Behav Sci (Basel). 2024 Jan 15;14(1):55. doi: 10.3390/bs14010055. Behav Sci (Basel). 2024. PMID: 38247707 Free PMC article.
References
-
- Akselrod M, Martuzzi R, Serino A, van der Zwaag W, Gassert R, Blanke O. Anatomical and functional properties of the foot and leg representation in areas 3b, 1 and 2 of primary somatosensory cortex in humans: A 7T fMRI study. Neuroimage 2017;159:473–487. - PubMed
-
- Blanke O, Slater M, Serino A. Behavioral, Neural, and Computational Principles of Bodily Self-Consciousness. Neuron 2015;88(1):145–166. - PubMed
