

Multimorbidity, healthcare use and catastrophic health expenditure by households in India: a cross-section analysis of self-reported morbidity from national sample survey data 2017-18
- PMID: 36096819
- PMCID: PMC9469515
- DOI: 10.1186/s12913-022-08509-x
Multimorbidity, healthcare use and catastrophic health expenditure by households in India: a cross-section analysis of self-reported morbidity from national sample survey data 2017-18
Abstract
Background: The purpose of this research is to generate new evidence on the economic consequences of multimorbidity on households in terms of out-of-pocket (OOP) expenditures and their implications for catastrophic OOP expenditure.
Methods: We analyzed Social Consumption Health data from National Sample Survey Organization (NSSO) 75th round conducted in the year 2017-2018 in India. The sample included 1,13,823 households (64,552 rural and 49,271 urban) through a multistage stratified random sampling process. Prevalence of multimorbidity and related OOP expenditure were estimated. Using Coarsened Exact Matching (CEM) we estimated the mean OOP expenditure for individuals reporting multimorbidity and single morbidity for each episode of outpatient visits and hospital admission. We also estimated implications in terms of catastrophic OOP expenditure for households.
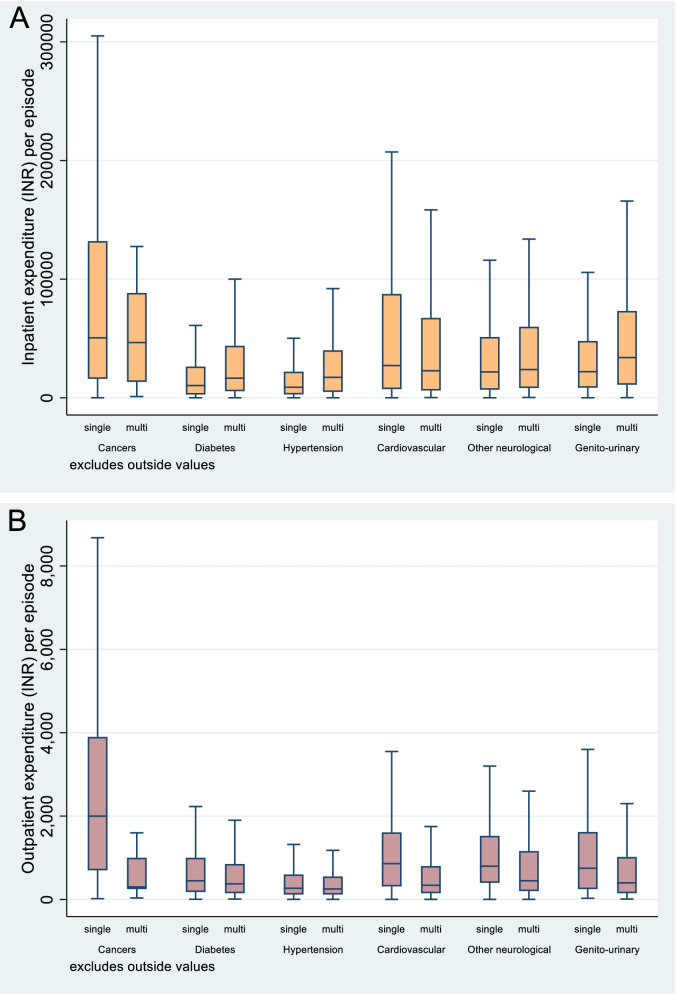
Results: Results suggest that outpatient OOP expenditure is invariably lower in the presence of multimorbidity as compared with single conditions of the selected Non-Communicable Diseases(NCDs) (overall, INR 720 [USD 11.3] for multimorbidity vs. INR 880 [USD 14.8] for single). In the case of hospitalization, the OOP expenditures were mostly higher for the same NCD conditions in the presence of multimorbidity as compared with single conditions, except for cancers and cardiovascular diseases. For cancers and cardiovascular, OOP expenditures in the presence of multimorbidity were lower by 39% and 14% respectively). Furthermore, around 46.7% (46.674-46.676) households reported incurring catastrophic spending (10% threshold) because of any NCD in the standalone disease scenario which rose to 63.3% (63.359-63.361) under the multimorbidity scenario. The catastrophic implications of cancer among individual diseases was the highest.
Conclusions: Multimorbidity leads to high and catastrophic OOP payments by households and treatment of high expenditure diseases like cancers and cardiovascular are under-financed by households in the presence of competing multimorbidity conditions. Multimorbidity should be considered as an integrated treatment strategy under the existing financial risk protection measures (Ayushman Bharat) to reduce the burden of household OOP expenditure at the country level.
Keywords: India; catastrophic expenditure; multimorbidity; out-of-pocket expenditure.
© 2022. The Author(s).
Conflict of interest statement
We declare no conflict of interest.
Figures
References
-
- Collaborators GBDRF Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1345–1422. doi: 10.1016/S0140-6736(17)32366-8. - DOI - PMC - PubMed
-
- Disease GBD, Injury I, Prevalence C. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1211–1259. doi: 10.1016/S0140-6736(17)32154-2. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
