

A neural stem cell paradigm of pediatric hydrocephalus
- PMID: 36097331
- PMCID: PMC10110448
- DOI: 10.1093/cercor/bhac341
A neural stem cell paradigm of pediatric hydrocephalus
Abstract
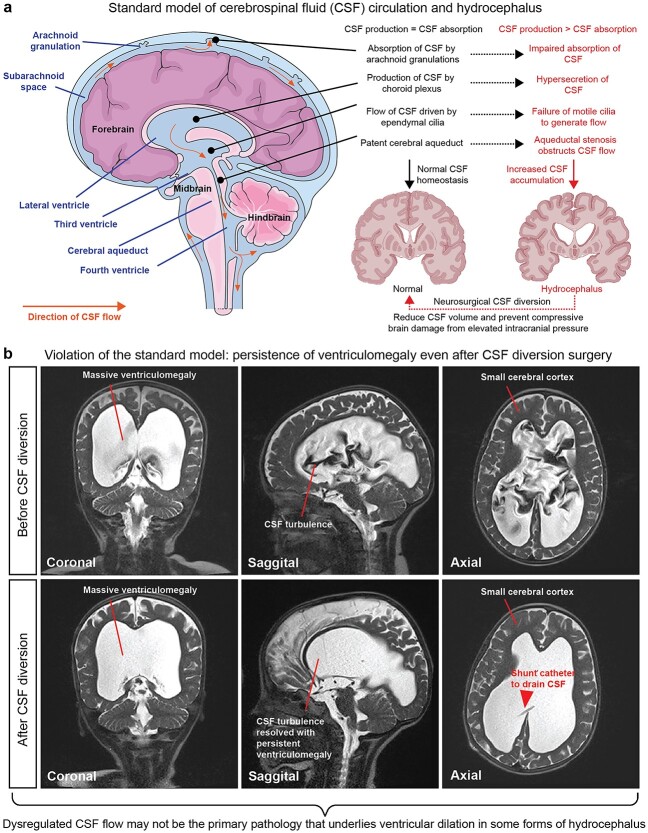
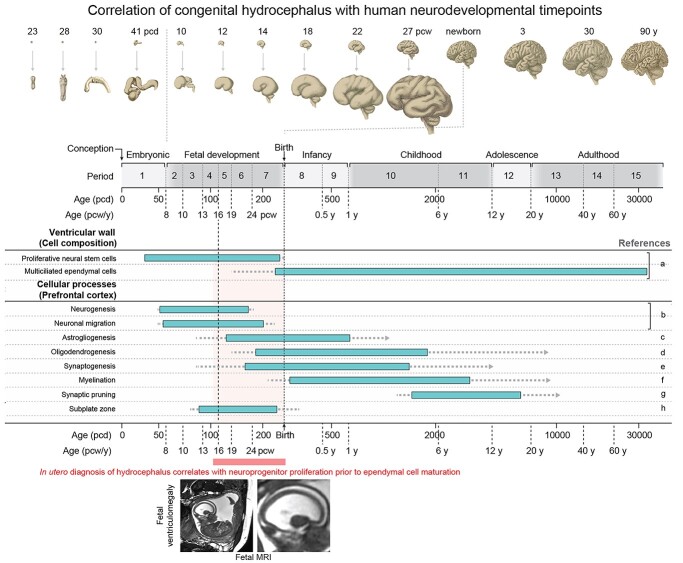
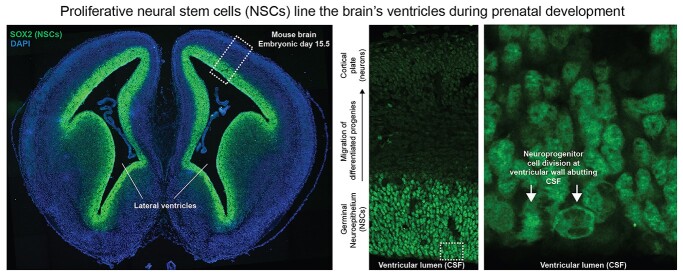
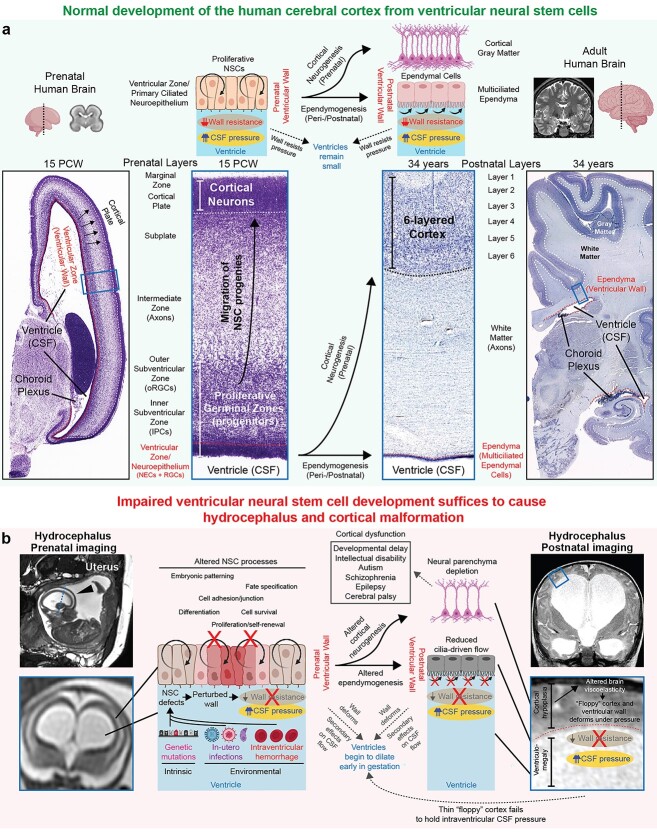
Pediatric hydrocephalus, the leading reason for brain surgery in children, is characterized by enlargement of the cerebral ventricles classically attributed to cerebrospinal fluid (CSF) overaccumulation. Neurosurgical shunting to reduce CSF volume is the default treatment that intends to reinstate normal CSF homeostasis, yet neurodevelopmental disability often persists in hydrocephalic children despite optimal surgical management. Here, we discuss recent human genetic and animal model studies that are shifting the view of pediatric hydrocephalus from an impaired fluid plumbing model to a new paradigm of dysregulated neural stem cell (NSC) fate. NSCs are neuroprogenitor cells that comprise the germinal neuroepithelium lining the prenatal brain ventricles. We propose that heterogenous defects in the development of these cells converge to disrupt cerebrocortical morphogenesis, leading to abnormal brain-CSF biomechanical interactions that facilitate passive pooling of CSF and secondary ventricular distention. A significant subset of pediatric hydrocephalus may thus in fact be due to a developmental brain malformation leading to secondary enlargement of the ventricles rather than a primary defect of CSF circulation. If hydrocephalus is indeed a neuroradiographic presentation of an inborn brain defect, it suggests the need to focus on optimizing neurodevelopment, rather than CSF diversion, as the primary treatment strategy for these children.
Keywords: cerebrospinal fluid; hydrocephalus; neural stem cell; neurodevelopmental disorders; neuroprogenitor.
© The Author(s) 2022. Published by Oxford University Press. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Adle-Biassette H, Saugier-Veber P, Fallet-Bianco C, Delezoide A-LL, Razavi F, Drouot N, Bazin A, Beaufrère A-M, Bessières B, Blesson S, et al. Neuropathological review of 138 cases genetically tested for X-linked hydrocephalus: evidence for closely related clinical entities of unknown molecular bases. Acta Neuropathol. 2013:126(3):427–442. 10.1007/s00401-013-1146-1. - DOI - PubMed
-
- Allocco AA, Jin SC, Duy PQ, Furey CG, Zeng X, Dong W, Nelson-Williams C, Karimy JK, DeSpenza T, Hao LT, et al. Recessive inheritance of congenital hydrocephalus with other structural brain abnormalities caused by compound heterozygous mutations in ATP1A3. Front Cell Neurosci. 2019:13:425. 10.3389/fncel.2019.00425. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
