

A comparative evaluation of fixed dose and separately administered combinations of lisinopril and hydrochlorothiazide in treatment-naïve adult hypertensive patients in a rural Nigerian community
- PMID: 36097516
- PMCID: PMC9463461
- DOI: 10.1016/j.ijcrp.2022.200144
A comparative evaluation of fixed dose and separately administered combinations of lisinopril and hydrochlorothiazide in treatment-naïve adult hypertensive patients in a rural Nigerian community
Abstract
Background: Antihypertensive drugs administered as fixed dose combination (FDC) therapy compared to separately administered combination therapy have been proposed to improve treatment compliance/adherence, and therefore the efficacy of blood pressure (BP) control treatment.
Aim: The aim of this present study is to compare the blood pressure control, renal end-organ protection and medication compliance/adherence in patients receiving FDC and those receiving separately administered combinations of Lisinopril and Hydrochlorothiazide in treatment-naive hypertensive adult patients in a rural Nigerian community.
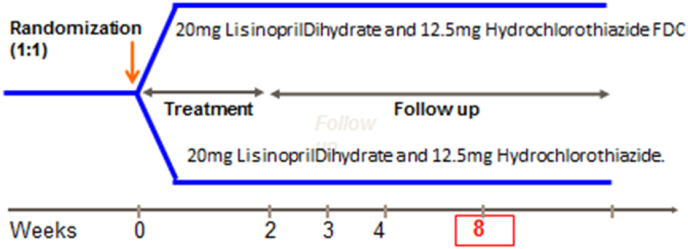
Method: ology: This randomized two-arm prospective longitudinal 8-week parallel-group study was carried-out for 6-month at the Ajegunle Community between April 2018 and October 2018. Efficacy variables included the changes from baseline in mean sitting systolic BP (MSSBP) and mean sitting diastolic BP (MSDBP). Medication safety, compliance/adherence and renal end-organ protection were assessed.
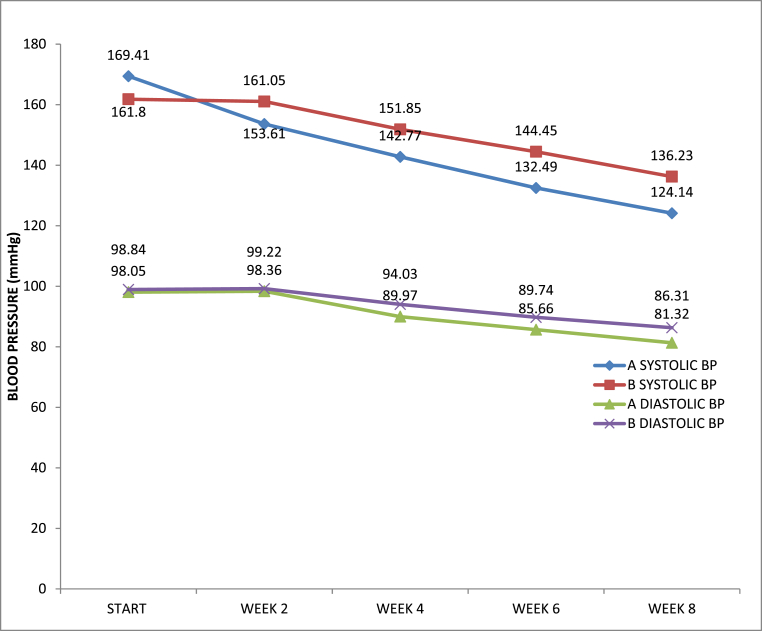
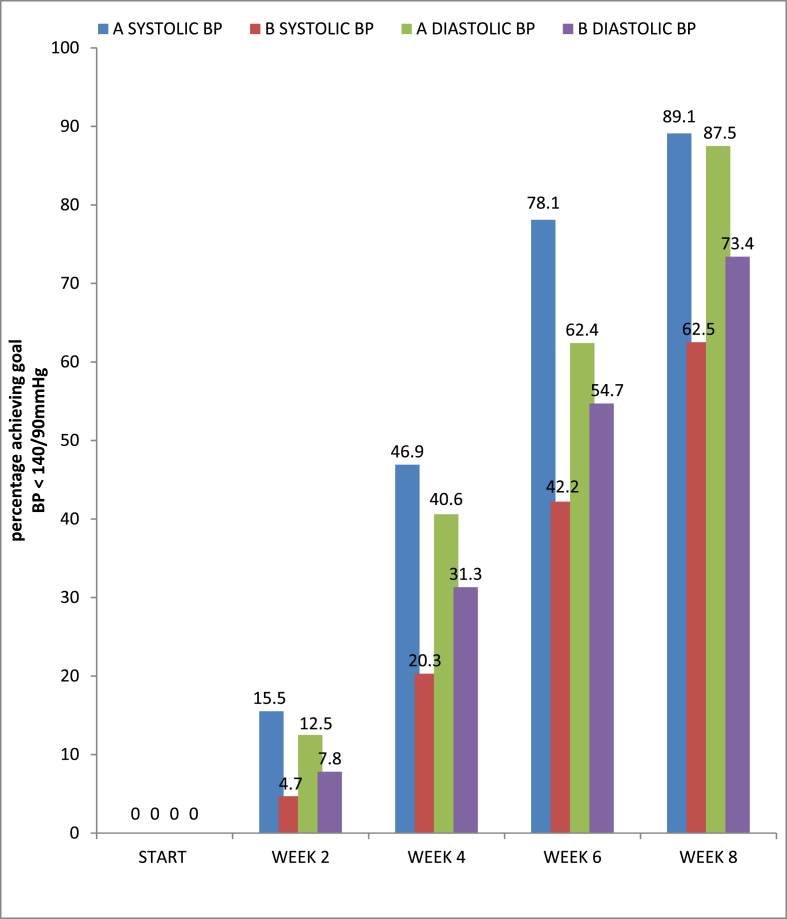
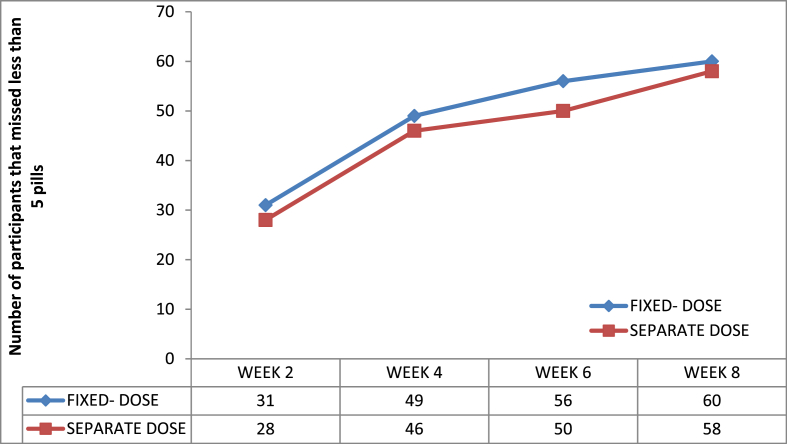
Results: The baseline characteristics of the two groups were similar. Prevalence of hypertension was found to be 32.9%. The mean blood pressure of all the participants was 165.6 ± 16.5 mmHg and 98.5 ± 11.5 mmHg for systolic BP and diastolic BP respectively, while the mean pulse rate of the participants was 85.0 ± 13.4 beats/min. At the 8-week end point, both regimens had achieved significant reductions from baseline in MSSBP (-33.18 and -37.16 mm Hg, respectively; both, P < 0.05) and MSDBP (-12.97 and -17.53 mm Hg; both, P < 0.05). Both regimens were generally well tolerated. Adherence was better in the FDC arm and there was no any reported case of proteinuria occurrence in both arms.
Conclusion: The high prevalence of hypertension in the community shows that there is unmet need in diagnosis and awareness of the disease. Both combination therapies were well tolerated; but the FDC antihypertensive therapy resulted in statistically significant amount of BP reductions than the separately administered combination antihypertensive therapy. Making FDCs available and affordable will help many hypertensive patients to achieve their target BP control goals easily.
Keywords: Ajegunle community; BP:, Blood Pressure; FDC:, Fixed Dose Combination; Fixed-dose combination antihypertensive therapy; Hydrochlorothiazide; Lisinopril; MSDBP:, Mean Sitting DiastolicBlood Pressure; MSSBP:, Mean Sitting SystolicBlood Pressure; Nigeria; Separately administered combination antihypertensive therapy; Treatment-naive hypertensive adult patients.
© 2022 The Authors.
Conflict of interest statement
None to declare; as there is no any conflict of interest among the authors.
Figures
References
-
- Salako B.L. Blood pressure control in sub-Saharan Africans: a physician's perspectives. Postgrad. Doc. Afr. 2003;25:4–7.
-
- Adeloye D., Basquill C., Aderemi A.V., Thompson J.Y., Obi F.A. An estimate of the prevalence of hypertension in Nigeria: a systemic review and meta-analysis. J. Hypert. 2015;32:230–424. - PubMed
-
- Gup Ilo, Amadi A.N. Essential hypertension in adult Nigerians in a primary care clinic: a cross-sectional study of the prevalence and associated family socio-biological factors in Eastern Nigeria. Eur. J. Prev. Med. 2014;2(6):81–89.
-
- Ukwe C.V., Ubaka C.M. Antihypertensive drug prescribing in a tertiary hospital in Eastern Nigeria. Trop. J. Pharmaceut. Res. 2012;11(2):297.
LinkOut - more resources
Full Text Sources
Miscellaneous