

Non-Invasive Assessment of Intracranial Hypertension in Patients with Traumatic Brain Injury Using Computed Tomography Radiomic Features: A Pilot Study
- PMID: 36097763
- PMCID: PMC9902045
- DOI: 10.1089/neu.2022.0277
Non-Invasive Assessment of Intracranial Hypertension in Patients with Traumatic Brain Injury Using Computed Tomography Radiomic Features: A Pilot Study
Abstract
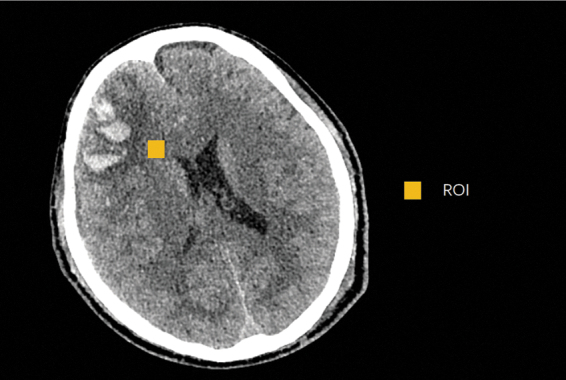
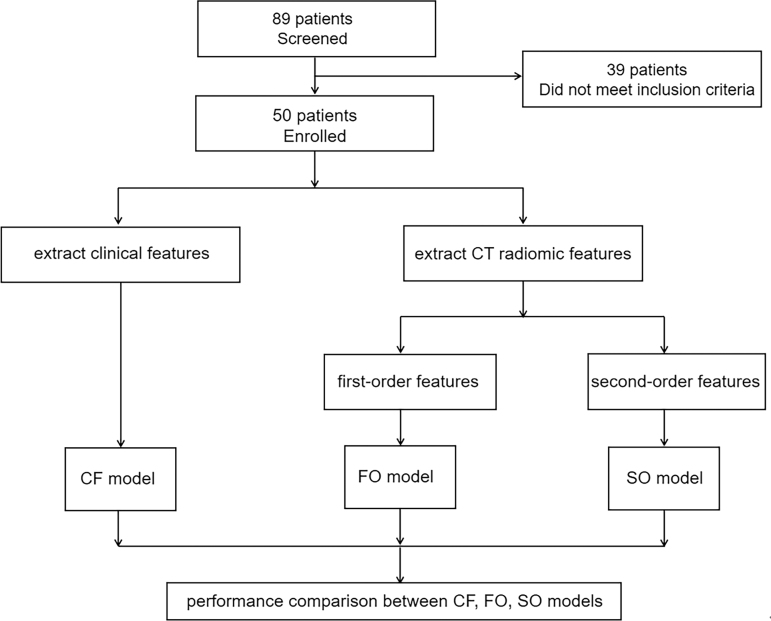
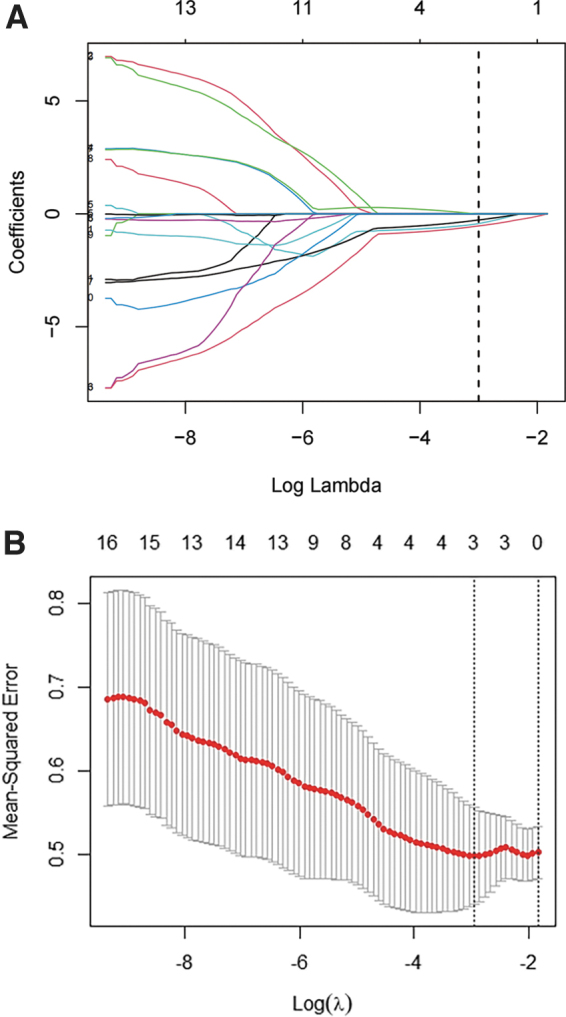
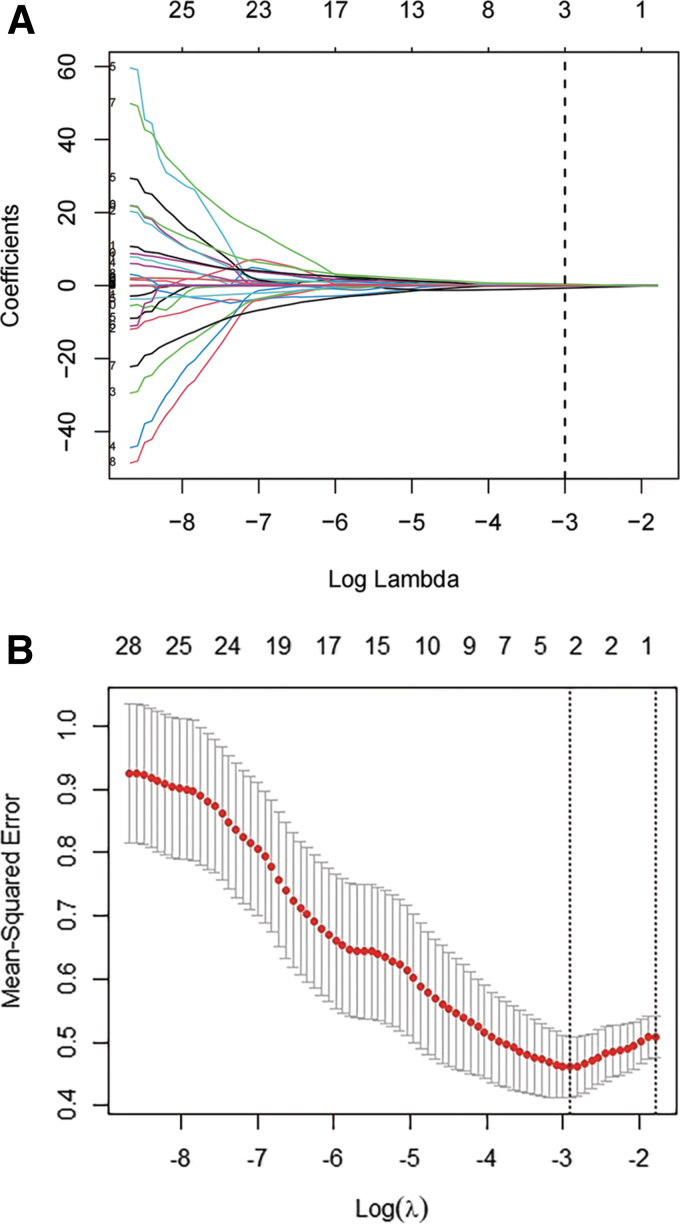
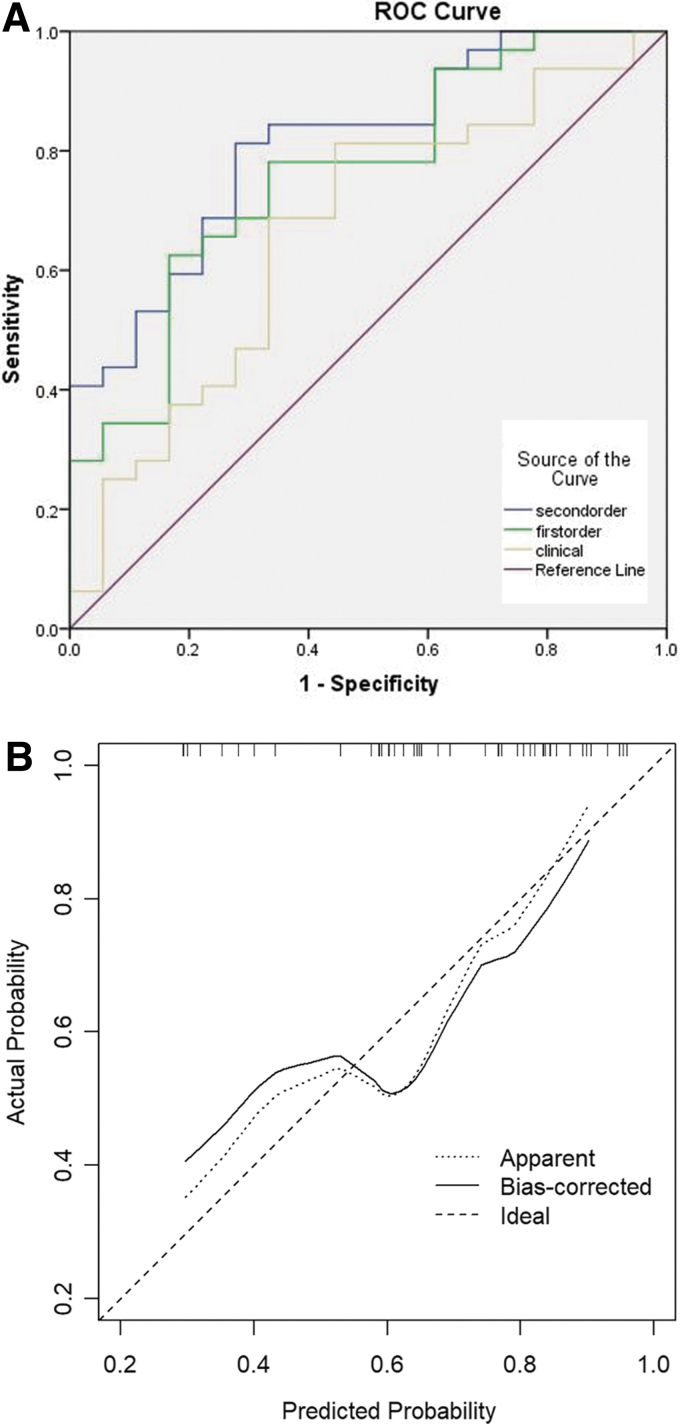
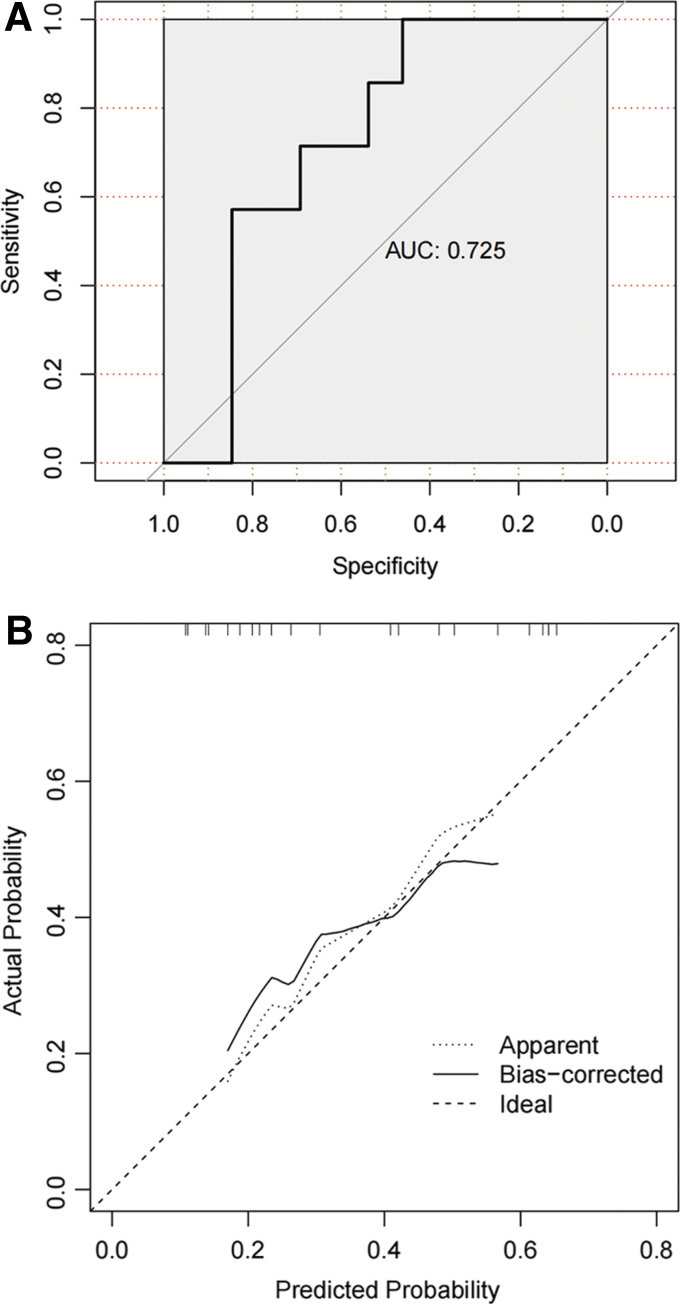
This study aimed to assess intracranial hypertension in patients with traumatic brain injury non-invasively using computed tomography (CT) radiomic features. Fifty patients from the primary cohort were enrolled in this study. The clinical data, pre-operative cranial CT images, and initial intracranial pressure readings were collected and used to develop a prediction model. Data of 20 patients from another hospital were used to validate the model. Clinical features including age, sex, midline shift, basilar cistern status, and ventriculocranial ratio were measured. Radiomic features-i.e., 18 first-order and 40 second-order features- were extracted from the CT images. LASSO method was used for features filtration. Multi-variate logistic regression was used to develop three prediction models with clinical (CF model), first-order (FO model), and second-order features (SO model). The SO model achieved the most robust ability to predict intracranial hypertension. Internal validation showed that the C-statistic of the model was 0.811 (95% confidence interval [CI]: 0.691-0.931) with the bootstrapping method. The Hosmer Lemeshow test and calibration curve also showed that the SO model had excellent performance. The external validation results showed a good discrimination with an area under the curve of 0.725 (95% CI: 0.500-0.951). Although the FO model was inferior to the SO model, it had better prediction ability than the CF model. The study shows that the radiomic features analysis, especially second-order features, can be used to evaluate intracranial hypertension non-invasively compared with conventional clinical features, given its potential for clinical practice and further research.
Keywords: computed tomography; intracranial hypertension; radiomics; traumatic brain injury.
Conflict of interest statement
No competing financial interests exist.
Figures
Similar articles
-
Development and validation of intracranial hypertension prediction models based on radiomic features in patients with traumatic brain injury: an exploratory study based on CENTER-TBI data.Crit Care. 2025 Mar 6;29(1):100. doi: 10.1186/s13054-025-05328-4. Crit Care. 2025. PMID: 40050978 Free PMC article.
-
Initial CT-based radiomics nomogram for predicting in-hospital mortality in patients with traumatic brain injury: a multicenter development and validation study.Neurol Sci. 2022 Jul;43(7):4363-4372. doi: 10.1007/s10072-022-05954-8. Epub 2022 Feb 24. Neurol Sci. 2022. PMID: 35199252
-
Poor Accuracy of Manually Derived Head Computed Tomography Parameters in Predicting Intracranial Hypertension After Nontraumatic Intracranial Hemorrhage.Neurocrit Care. 2023 Dec;39(3):677-689. doi: 10.1007/s12028-022-01662-5. Epub 2022 Dec 28. Neurocrit Care. 2023. PMID: 36577900
-
Prediction of Early Intracranial Hypertension After Severe Traumatic Brain Injury: A Prospective Study.World Neurosurg. 2019 Jul;127:e1242-e1248. doi: 10.1016/j.wneu.2019.04.121. Epub 2019 Apr 19. World Neurosurg. 2019. PMID: 31009774
-
Ratio of Optic Nerve Sheath Diameter to Eyeball Transverse Diameter by Ultrasound Can Predict Intracranial Hypertension in Traumatic Brain Injury Patients: A Prospective Study.Neurocrit Care. 2020 Apr;32(2):478-485. doi: 10.1007/s12028-019-00762-z. Neurocrit Care. 2020. PMID: 31218637
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
