

Influence of different region of interest sizes on CT-based radiomics model for microvascular invasion prediction in hepatocellular carcinoma
- PMID: 36097772
- PMCID: PMC10950113
- DOI: 10.11817/j.issn.1672-7347.2022.220027
Influence of different region of interest sizes on CT-based radiomics model for microvascular invasion prediction in hepatocellular carcinoma
Abstract
Objectives: Microvascular invasion (MVI) is an important predictor of postoperative recurrence or poor outcomes of hepatocellular carcinoma (HCC). Radiomics is able to predict MVI in HCC preoperatively. This study aims to investigate the influence of different region of interest (ROI) sizes on CT-based radiomics model for MVI prediction in HCC.
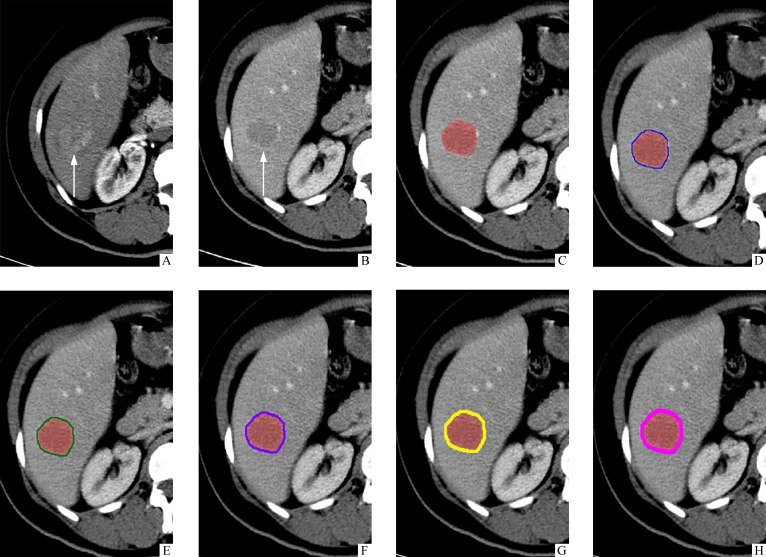
Methods: Patients with HCC with or without MVI confirmed by pathology and those who underwent preoperative plain or enhanced abdominal CT scans in the Third Xiangya Hospital of Central South University from January 2010 to December 2020 were retrospectively and consecutively included. According to the ratio of 7 to 3, the patients were randomly assigned into a training set and a validation set. Clinical data were collected from medical records, and radiomics features were extracted from the arterial phase (AP) and portal venous phase (PVP) of preoperatively acquired CT in all patients. Six different ROI sizes were employed. The original ROI (OROI) was manually delineated along the visible borders of the tumor layer-by-layer. The OROI was expanded out by 1-5 mm. The OROI was combined with 5 different peritumoral regions to generate the other 5 ROIs, named Plus1-Plus5. Feature extraction, dimension reduction, and model development were conducted in 6 different ROIs separately. Supporter vector machine (SVM) was used for model construction. Model performance was assessed via receiver operating characteristic (ROC) curve.
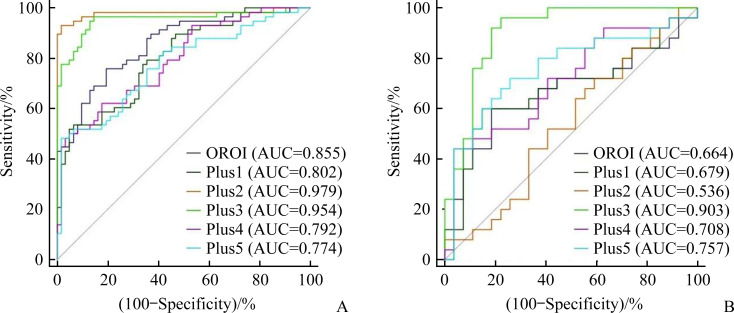
Results: A total of 172 HCC patients were included, in which 83 (48.3%) were MVI positive, and 89 (51.7%) were MVI negative. Three hundred and ninety-six features based on AP or PVP images were extracted from each ROI. After feature selection and dimension reduction, 4, 5, 15, 11, 6, and 3 features of OROI, Plus1, Plus2, Plus 3, Plus4, and Plus5 were selected for model construction, respectively. In the training set, the sensitivity, specificity, and area under the curve (AUC) of OROI were 0.759, 0.806, and 0.855, respectively. The AUC values of Plus2 (0.979) and Plus3 (0.954) were higher than that of OROI. The AUC values of Plus1 (0.802), Plus4 (0.792), and Plus5 (0.774) were not significantly different from those of OROI. In the validation set, the sensitivity, specificity, and AUC value of OROI were 0.640, 0.630, and 0.664, respectively. The AUC value of Plus3 was 0.903, which was higher than that of OROI. The AUC values of Plus1 (0.679), Plus2 (0.536), Plus4 (0.708), and Plus5 (0.757) were not significantly different from that of OROI (P>0.05).
Conclusions: The size of ROI significantly inflluences on the performance of CT-based radiomics model for MVI prediction in HCC. Including appropriate area around the tumor into ROI could improve the predictive performance of the model, and 3 mm might be appropriate distance.
目的: 微血管侵犯(microvascular invasion,MVI)是肝细胞癌(hepatocellular carcinoma,HCC)术后复发和预后不良的重要预测因子。影像组学能在术前预测HCC是否存在MVI。本研究探讨不同感兴趣区(region of interest,ROI)范围对基于CT影像组学模型预测HCC有无 MVI的影响。方法: 回顾性连续收集中南大学湘雅三医院2010年1月至2020年12月间经手术病理证实为HCC,且在术前进行过腹部CT平扫或增强扫描的患者。患者以7꞉3的比例随机分为训练组和验证组。根据病理报告评估患者的MVI情况。在动脉期及门脉期CT图像上手动逐层沿肿瘤边缘勾画ROI,命名为原始感兴趣区(original region of interest,OROI),然后由软件自动向外扩展1~5 mm。OROI分别与瘤周1~5 mm区域联合生成5个ROI,分别命名为Plus1~Plus5。分别提取以上6个ROI的影像组学特征,经过特征选择及数据降维筛选出有预测价值的特征,通过支持向量机(supporter vector machine,SVM)分别构建6个影像组学模型。对各模型的预测效能进行受试者工作特征(receiver operating characteristic,ROC)曲线分析。结果: 纳入172名HCC患者,其中83名(48.3%)MVI阳性,89名(51.7%)MVI阴性。从动脉期及门脉期分别提取396个特征,经过特征选择及降维,OROI、Plus1~Plus5分别有4、5、15、11、6、3个特征被选择用于建模。在训练组中,OROI的灵敏度、特异度及曲线下面积(area under the curve,AUC)分别为0.759、0.806和0.855。Plus2(AUC=0.979)及Plus3(AUC=0.954)的AUC高于OROI。Plus1(AUC=0.802)、Plus4(AUC=0.792)及Plus5(AUC=0.774)与OROI的AUC差异无统计学意义。在验证组中,OROI的灵敏度、特异度及AUC分别为0.640、0.630 和0.664。Plus3的AUC(0.903)高于OROI。Plus1(AUC=0.679)、Plus2(AUC=0.536)、Plus4(AUC=0.708)及Plus5(AUC=0.757)与OROI的AUC差异无统计学意义(P>0.05)。结论: ROI范围对CT影像组学模型预测HCC有无MVI有显著影响,将肿瘤外一定范围的肝组织包含在ROI内可能提高模型的预测效能,向瘤外扩展3 mm可能为最佳范围。.
Keywords: computed tomography; hepatocellular carcinoma; microvascular invasion; radiomics; region of interest.
Conflict of interest statement
作者声称无任何利益冲突。
Figures
Similar articles
-
Preoperative radiomics nomogram for microvascular invasion prediction in hepatocellular carcinoma using contrast-enhanced CT.Eur Radiol. 2019 Jul;29(7):3595-3605. doi: 10.1007/s00330-018-5985-y. Epub 2019 Feb 15. Eur Radiol. 2019. PMID: 30770969
-
[Value of the application of enhanced CT radiomics and machine learning in preoperative prediction of microvascular invasion in hepatocellular carcinoma].Zhonghua Yi Xue Za Zhi. 2021 May 11;101(17):1239-1245. doi: 10.3760/cma.j.cn112137-20200820-02425. Zhonghua Yi Xue Za Zhi. 2021. PMID: 34865392 Clinical Trial. Chinese.
-
Considerable effects of imaging sequences, feature extraction, feature selection, and classifiers on radiomics-based prediction of microvascular invasion in hepatocellular carcinoma using magnetic resonance imaging.Quant Imaging Med Surg. 2021 May;11(5):1836-1853. doi: 10.21037/qims-20-218. Quant Imaging Med Surg. 2021. PMID: 33936969 Free PMC article.
-
Radiomics models for preoperative prediction of microvascular invasion in hepatocellular carcinoma: a systematic review and meta-analysis.Abdom Radiol (NY). 2022 Jun;47(6):2071-2088. doi: 10.1007/s00261-022-03496-3. Epub 2022 Apr 1. Abdom Radiol (NY). 2022. PMID: 35364684
-
Radiomics for the Preoperative Evaluation of Microvascular Invasion in Hepatocellular Carcinoma: A Meta-Analysis.Front Oncol. 2022 Apr 7;12:831996. doi: 10.3389/fonc.2022.831996. eCollection 2022. Front Oncol. 2022. PMID: 35463303 Free PMC article.
Cited by
-
Impact of deep learning image reconstruction algorithms on CT radiomic features in patients with liver tumors.Front Oncol. 2023 Apr 5;13:1167745. doi: 10.3389/fonc.2023.1167745. eCollection 2023. Front Oncol. 2023. PMID: 37091167 Free PMC article.
-
Prediction of Ki-67 expression in hepatocellular carcinoma with machine learning models based on intratumoral and peritumoral radiomic features.World J Gastrointest Oncol. 2025 May 15;17(5):104172. doi: 10.4251/wjgo.v17.i5.104172. World J Gastrointest Oncol. 2025. PMID: 40487953 Free PMC article.
-
Performance of Radiomics in Microvascular Invasion Risk Stratification and Prognostic Assessment in Hepatocellular Carcinoma: A Meta-Analysis.Cancers (Basel). 2023 Jan 25;15(3):743. doi: 10.3390/cancers15030743. Cancers (Basel). 2023. PMID: 36765701 Free PMC article. Review.
-
A new model based on preoperative AFP, albumin, and tumor burden score for predicting microvascular invasion in early-stage HCC.Am J Cancer Res. 2024 Oct 15;14(10):4979-4988. doi: 10.62347/ZGRJ7827. eCollection 2024. Am J Cancer Res. 2024. PMID: 39553207 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
