

Diagnostic Performance of Core Needle Biopsy for Characterizing Thyroidectomy Bed Lesions
- PMID: 36098339
- PMCID: PMC9523230
- DOI: 10.3348/kjr.2021.0772
Diagnostic Performance of Core Needle Biopsy for Characterizing Thyroidectomy Bed Lesions
Abstract
Objective: Thyroidectomy bed lesions frequently show suspicious ultrasound (US) features after thyroid surgery. Fine-needle aspiration (FNA) may not provide definitive pathological information about the lesions. Although core-needle biopsy (CNB) has excellent diagnostic performance in characterizing suspicious thyroid nodules, no published studies have evaluated the performance of CNB specifically for thyroidectomy bed lesions. Therefore, we aimed to evaluate the diagnostic performance and safety of CNB for characterizing thyroidectomy bed lesions.
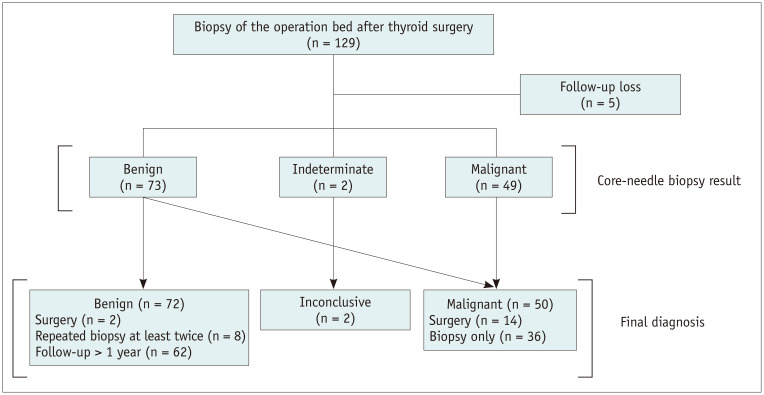
Materials and methods: A total of 124 thyroidectomy bed lesions in 113 patients (79 female and 34 male; age, 23-85 years) who underwent US-guided CNB between December 2008 and December 2020 were included. We reviewed the US imaging features of the target lesions and the histories of previous biopsies. The pathologic results, diagnostic performance for malignancy, and complications of CNB were analyzed.
Results: All samples (100%) obtained by CNB were adequate for pathological analysis. Pathological analysis revealed inconclusive results in two lesions (1.6%). According to the reference standard, 50 lesions were ultimately malignant (40.3%), and 72 were benign (58.1%), excluding the two inconclusive lesions. The performance of CNB for diagnosing malignant thyroidectomy bed lesions in the 122 lesions had a sensitivity of 98.0% (49/50), a specificity of 100% (72/72), positive predictive value of 100% (49/49), and negative predictive value of 98.6% (72/73). Eleven lesions were referred for CNB after prior inconclusive FNA results in thyroidectomy bed lesions, for all of which CNB yielded correct conclusive pathologic diagnoses. According to the pathological analysis of CNB, there were various benign lesions (58.9%, 73/124) besides recurrence, including benign postoperative lesions other than suture granuloma (32.3%, 40/124), suture granuloma (15.3%, 19/124), remnant thyroid tissue (5.6%, 7/124), parathyroid lesions (4%, 5/124), and abscesses (1.6%, 2/124). No major or minor complications were associated with the CNB procedure.
Conclusion: US-guided CNB is accurate and safe for characterizing thyroidectomy bed lesions.
Keywords: Core-needle biopsy; Fine-needle aspiration; Thyroid; Thyroid cancer; Thyroidectomy; Ultrasonography.
Copyright © 2022 The Korean Society of Radiology.
Conflict of interest statement
Jung Hwan Baek and Jeong Hyun Lee who is on the editorial board of the <i>Korean Journal of Radiology</i> was not involved in the editorial evaluation or decision to publish this article. All remaining authors have declared no conflicts of interest.
Figures
References
-
- Burgess JR, Tucker P. Incidence trends for papillary thyroid carcinoma and their correlation with thyroid surgery and thyroid fine-needle aspirate cytology. Thyroid. 2006;16:47–53. - PubMed
-
- do Rosário PW, Fagundes TA, Maia FF, Franco AC, Figueiredo MB, Purisch S. Sonography in the diagnosis of cervical recurrence in patients with differentiated thyroid carcinoma. J Ultrasound Med. 2004;23:915–920. quiz 921-922. - PubMed
-
- Lee YH, Lee NJ, Kim JH, Song JJ. US diagnosis of cervical recurrence in patients operated on thyroid cancer: sonographic features and clinical significance. Auris Nasus Larynx. 2007;34:213–219. - PubMed
-
- Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, et al. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid. 2016;26:1–133. - PMC - PubMed
-
- Bishop JA, Owens CL, Shum CH, Ali SZ. Thyroid bed fine-needle aspiration: experience at a large tertiary care center. Am J Clin Pathol. 2010;134:335–339. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
