

Mirabegron and antimuscarinic use in frail overactive bladder patients in the United States Medicare population
- PMID: 36098417
- PMCID: PMC9826123
- DOI: 10.1002/nau.25040
Mirabegron and antimuscarinic use in frail overactive bladder patients in the United States Medicare population
Abstract
Introduction: Overactive bladder (OAB) and frailty are independently associated with patient burden. However, economic burden and treatment-taking behavior have not been well characterized among frail patients with OAB, which, given the varying safety and tolerability profiles of available treatments, is crucial.
Objectives: To assess costs, health care resource utilization, treatment-taking behavior (persistence and adherence) to OAB medication in older, frail OAB patients.
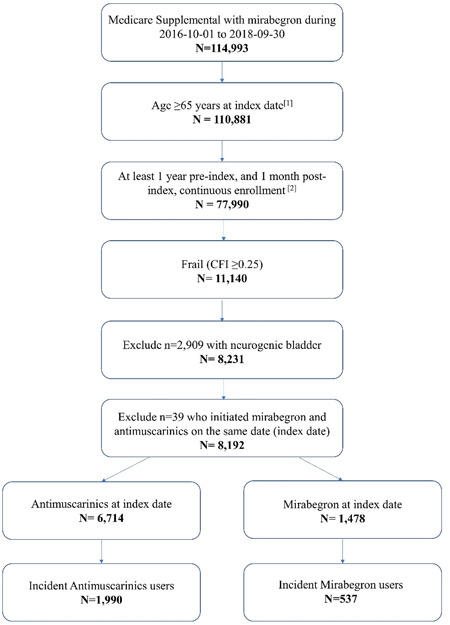
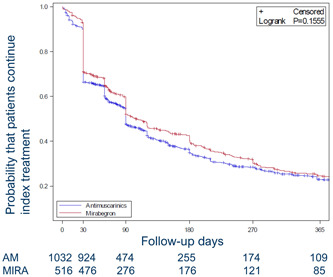
Methods: This was a retrospective cohort study using international business machines MarketScan Medicare Supplemental claims data. Eligible frail patients (per Claims-based Frailty Index score) initiating mirabegron were 1:2 propensity score matched (based on age, sex, and other characteristics) with those initiating antimuscarinics and were followed up to 1 year. All-cause, per-person, per-month costs, health care encounters, persistence (median days to discontinuation assessed using Kaplan-Meier methods) and adherence (≥80% of proportion of days covered at Day 365) were compared.
Results: From 2527 patients with incident mirabegron (21%) or antimuscarinic (79%) dispensations, 516 incident mirabegron users (median age: 82 years, 64% female) were matched to 1032 incident antimuscarinic users (median age: 81 years, 62% female). Median cost was higher in mirabegron group ($1581 vs. $1197 per month); this was primarily driven by medication cost. There was no difference in medical encounters. Adherence (39.1% vs. 33.8%) and persistence (103 vs. 90 days) were higher in mirabegron users.
Conclusions: Among frail older adults with OAB, mirabegron use was associated with higher costs and potential improvements in treatment-taking behaviors, particularly with respect to treatment adherence, versus those initiating antimuscarinics.
Keywords: adherence; costs; frail; health care resource utilization; persistence.
© 2022 The Authors. Neurourology and Urodynamics published by Wiley Periodicals LLC.
Conflict of interest statement
All authors all fulfill the ICMJE guidelines for authorship. D. W. and A. L. are employees of Astellas Pharma Global Development and T. K., D. N., and B. J., of Astellas Pharma US. T. M. J. received consulting fees from Astellas for the conduct of this study, as well as research support from Medtronic and Dexcom, consultation fees from Eisai, and authorship royalties from UpToDate. G. L. O. is an employee of Broadstreet HEOR which received a contract for consultant services for this study.
Figures
References
-
- Abrams P, Andersson KE, Apostolidis A, et al. International consultation on incontinence. recommendations of the international scientific committee: evaluation and treatment of urinary incontinence, pelvic organ prolapse and faecal incontinence. Neurourol Urodyn. 2018;37(7):2271‐2272. 10.1002/nau.23551 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
