

Is Hip Medial Ultrasound More Accurate Than Radiography for Determining the Status of Hip Reduction in Children Treated With a Spica Cast? A Retrospective Diagnostic Accuracy Study
- PMID: 36099306
- PMCID: PMC9928857
- DOI: 10.1097/CORR.0000000000002366
Is Hip Medial Ultrasound More Accurate Than Radiography for Determining the Status of Hip Reduction in Children Treated With a Spica Cast? A Retrospective Diagnostic Accuracy Study
Abstract
Background: Developmental dysplasia of the hip (DDH) is the most common hip abnormality in children. Closed or open reduction and cast immobilization are the most commonly used treatments for patients aged 6 to 18 months with dislocation; they are also used in children younger than 6 months when brace treatment is not effective. During cast immobilization, surgeons need reliable and timely imaging methods to assess the status of hip reduction to ensure successful treatment and avoid complications. Several methods are used, but they have disadvantages. We developed and, in this study, evaluated a hip medial ultrasound method to evaluate the status of hip reduction in children treated with a spica cast.
Question/purpose: Is hip medial ultrasound more accurate than radiography for determining the status of hip reduction in children treated with a spica cast?
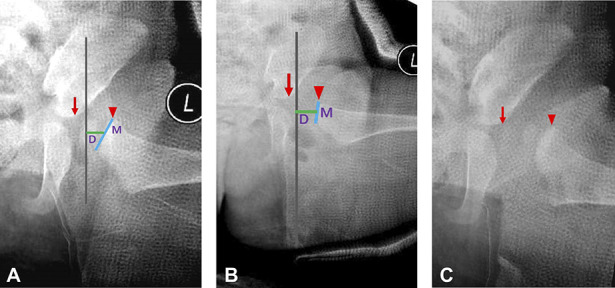
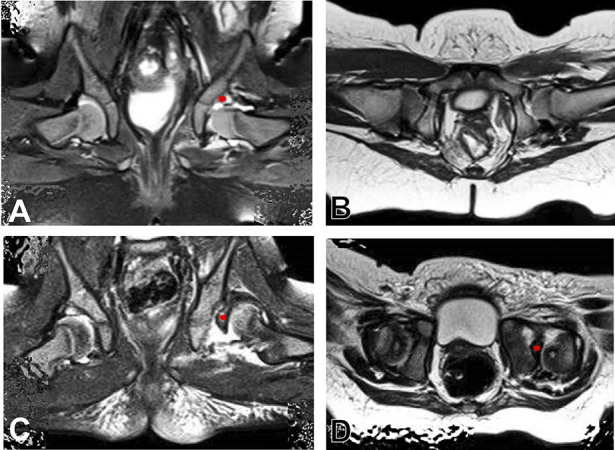
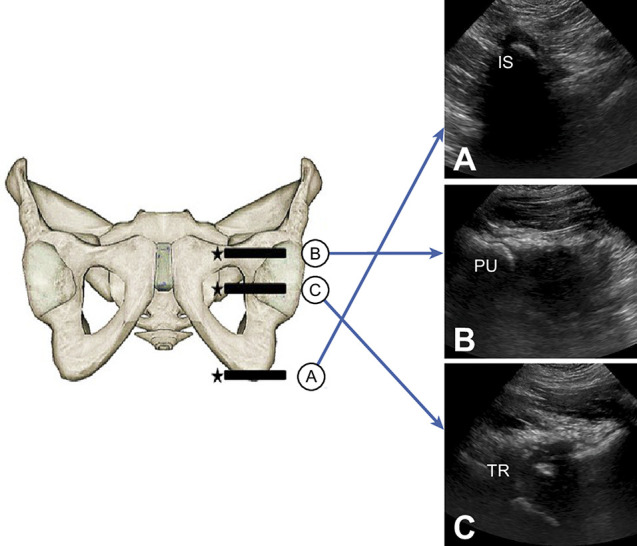
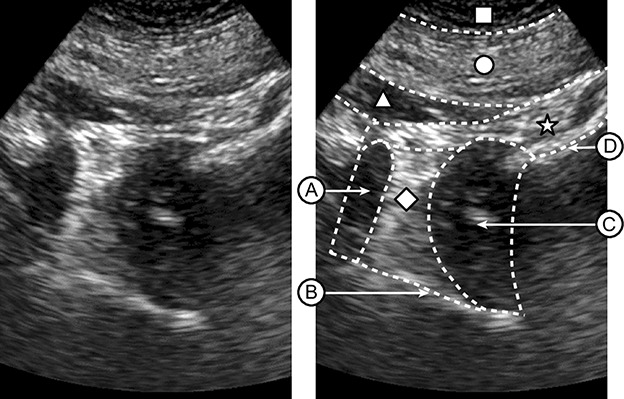
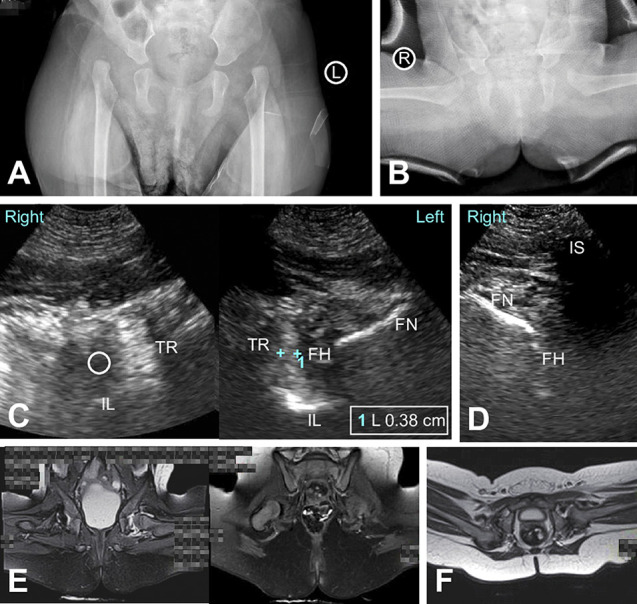
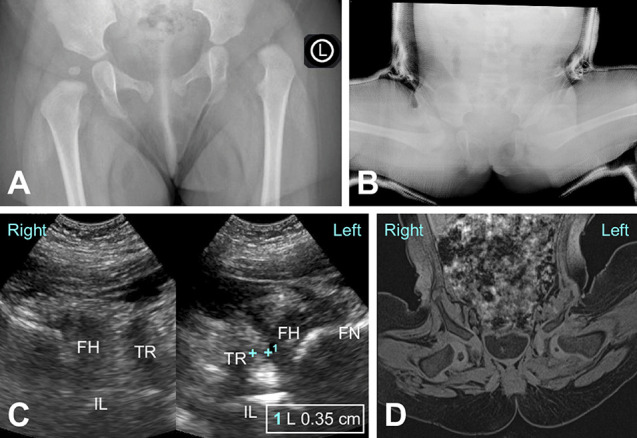
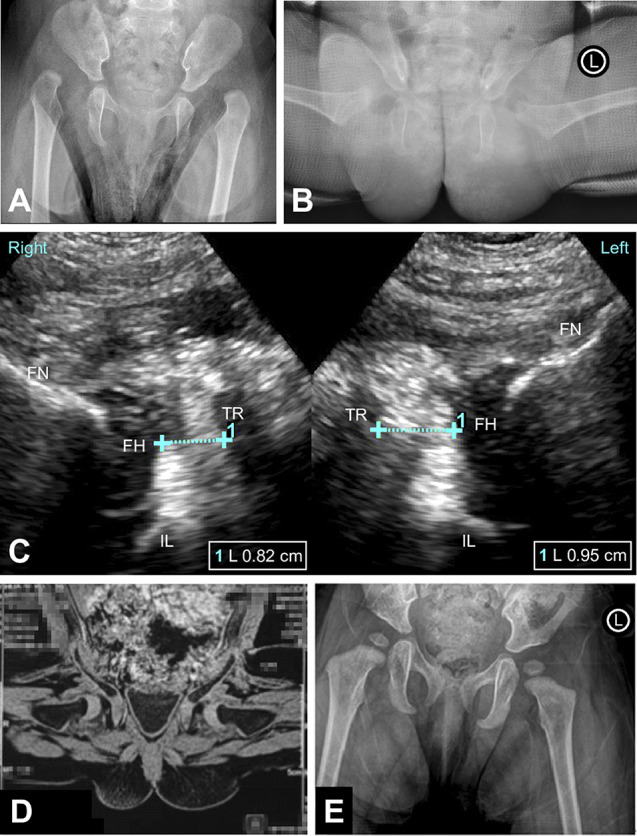
Methods: Between November 2017 and December 2020, we treated 136 patients with closed or open reduction and spica casting for DDH in our department. These children were 3 to 18 months old at the time of surgical reduction and had a specific medical history, physical examination findings, or AP radiographic evidence of unilateral or bilateral DDH. None had a concomitant femoral/acetabular osteotomy procedure in these hips. All patients underwent hip medial ultrasound, AP radiography, and MRI under sedation within 2 to 7 days after open or closed reduction. The examination time was from the second day after reduction to enable the patient to recover from anesthesia. MRI was performed within 7 days after reduction because of a few long appointment times, and ultrasound and AP radiography were always performed 1 or 2 days before MRI. Based on that, 65% (88 of 136 [88 hips]) of patients were excluded due to the absence of MRI, ultrasound, or AP radiography; 3% (4 of 136 [4 hips]) of patients were excluded because of concurrent congenital spina bifida, Larson syndrome, or Prader-Willi syndrome; and 1% (1 of 136 [1 hip]) of patients were excluded because the patient underwent MRI before ultrasound. A total of 32% (43 of 136 [43 hips]) of patients were eligible for analysis in this cross-sectional diagnostic study, and these 43 patients underwent AP radiography, ultrasound, and MRI. In this retrospective study, the mean age at the time of surgery was 10 ± 4 months (male:female ratio 5:38; unilateral DDH: 34; bilateral DDH: 9). To ensure the independence of the results, the study was limited to one hip per patient (in patients with bilateral DDH, the right hip was evaluated). The reduction of 43 hips (left:right ratio 26:17; closed:open reduction ratio 30:13) was evaluated by MRI, hip medial ultrasound, and radiography. Children with spica casts were placed in the supine position, which is necessary to expose the perineum for ultrasound. We used a broad-spectrum, microconvex, and intracavitary probe. The acetabular medial wall was identified by the triradiate cartilage of the ischial tuberosity and the pubis superior, and the femoral head was identified by the femoral neck. Then, the acetabulum coronal midsectional plane was used to determine the positions of the femoral head and acetabulum and to measure the triradiate cartilage-femoral distance. MRI examinations were performed using a 1.5-T MRI system with an eight-channel body coil. Each reviewer evaluated each reduction independently. Additionally, to further assess the hip medial ultrasound method's reliability and reproducibility, we investigated the interobserver and intraobserver agreement in evaluating the reduction using hip medial ultrasound. Using ultrasound or radiography, the reviewers classified hips as reduced, uncertain status, or dislocated. MRI was considered the gold standard for assessing hip reduction, and the reviewers classified hips as reduced or dislocated by MRI. Patients with hips with an uncertain reduction status according to ultrasound or radiography were retained in the analysis. Thus, the test results of radiography and ultrasound were classified into three classifications (positive, negative, or uncertain) in the present study. The test was considered positive or negative when patients were assessed with dislocation or without dislocation, respectively. The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) of ultrasound and radiography were calculated and compared. We combined uncertain and positive into the positive classification to be conservative in the statistical choices. The specificity, sensitivity, PPV, and NPV were analyzed based on this premise. Furthermore, a subgroup analysis was conducted by sex. MRI evaluation revealed that 41 hips were reduced and two hips were dislocated.
Results: The sensitivity, specificity, PPV, and NPV of ultrasound were 100% (95% CI 16% to 100%), 95% (95% CI 84% to 99%), 50% (95% CI 7% to 93%), and 100% (95% CI 91% to 100%), respectively. The sensitivity, specificity, PPV, and NPV of radiography were 50% (95% CI 1% to 99%), 68% (95% CI 52% to 82%), 7% (95% CI 0% to 34%), and 97% (95% CI 82% to 100%), respectively. Ultrasound showed a higher specificity (95% versus 68%; p < 0.001) and PPV (50% versus 7%; p = 0.02) than radiography. The sensitivity, specificity, PPV, and NPV of ultrasound were 100% (95% CI 16% to 100%), 94% (95% CI 81% to 99%), 50% (95% CI 7% to 93%), and 100% (95% CI 90% to 100%), respectively, for female patients (with only five male patients, we could not perform these analyses in this group). The sensitivity, specificity, PPV, and NPV of radiography were 50% (95% CI 1% to 99%), 64% (95% CI 46% to 79%), 7% (95% CI 0% to 34%), and 96% (95% CI 79% to 100%), respectively, for female patients. The κ values for intra- and interobserver reliability both were 1.0.
Conclusion: Hip medial ultrasound can directly visualize the femoral head and acetabulum. Hip medial ultrasound is more reliable than radiography as a preliminary evaluation method and does not involve irradiation. We recommend using hip medial ultrasound during outpatient follow-up visits for patients younger than 2 years treated with hip reduction and cast immobilization.
Level of evidence: Level III, diagnostic study.
Copyright © 2022 by the Association of Bone and Joint Surgeons.
Conflict of interest statement
Each author certifies that there are no funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article related to the author or any immediate family members. All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research® editors and board members are on file with the publication and can be viewed on request.
Figures

Comment in
-
CORR Insights®: Is Hip Medial Ultrasound More Accurate Than Radiography for Determining the Status of Hip Reduction in Children Treated With a Spica Cast? A Retrospective Diagnostic Accuracy Study.Clin Orthop Relat Res. 2023 Mar 1;481(3):606-607. doi: 10.1097/CORR.0000000000002416. Epub 2022 Sep 21. Clin Orthop Relat Res. 2023. PMID: 36135977 Free PMC article. No abstract available.
References
-
- Barrera CA, Cohen SA, Sankar WN, Ho-Fung VM, Sze RW, Nguyen JC. Imaging of developmental dysplasia of the hip: ultrasound, radiography and magnetic resonance imaging. Pediatr Radiol. 2019;49:1652-1668. - PubMed
-
- Dibello D, Odoni L, Pederiva F, Di Carlo V. MRI in post reduction evaluation of developmental dysplasia of the hip. J Pediatr Orthop. 2019;39:449-452. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
