

Sociodemographic Characteristics and Screening Outcomes of Women Preferring Self-Sampling in the Dutch Cervical Cancer Screening Programme: A Population-Based Study
- PMID: 36099416
- PMCID: PMC9900317
- DOI: 10.1158/1055-9965.EPI-22-0712
Sociodemographic Characteristics and Screening Outcomes of Women Preferring Self-Sampling in the Dutch Cervical Cancer Screening Programme: A Population-Based Study
Abstract
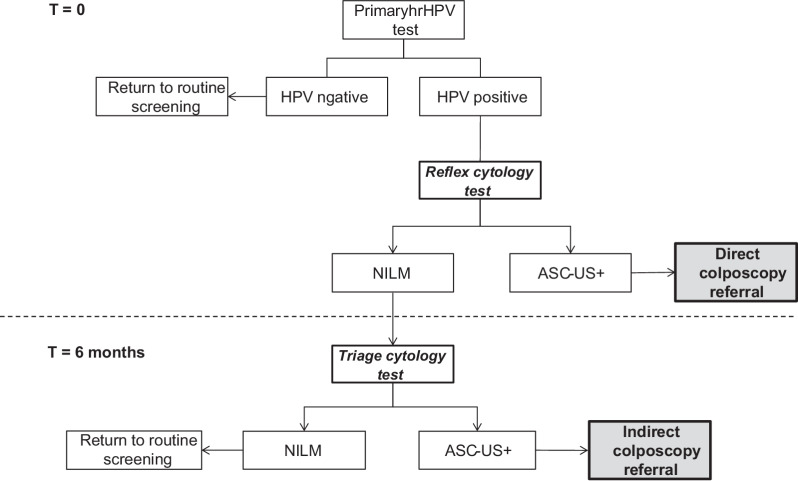
Background: In the Netherlands, lower high-risk human papillomavirus (hrHPV) positivity but higher cervical intraepithelial neoplasia (CIN) 2+ detection were found in self-collected compared with clinician-collected samples. To investigate the possible reason for these differences, we compared sociodemographic and screening characteristics of women and related these to screening outcomes.
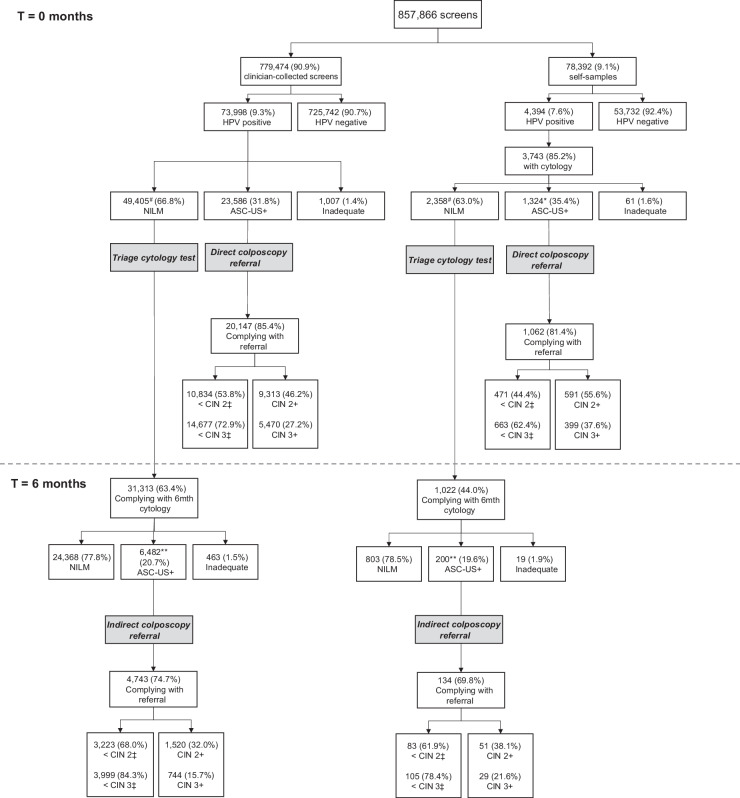
Methods: We extracted data from PALGA on all primary hrHPV screens and associated follow-up tests for 857,866 screened women, invited in 2017 and 2018. We linked these data with sociodemographic data from Statistics Netherlands. Logistic regression was performed for hrHPV positivity and CIN 2+/3+ detection.
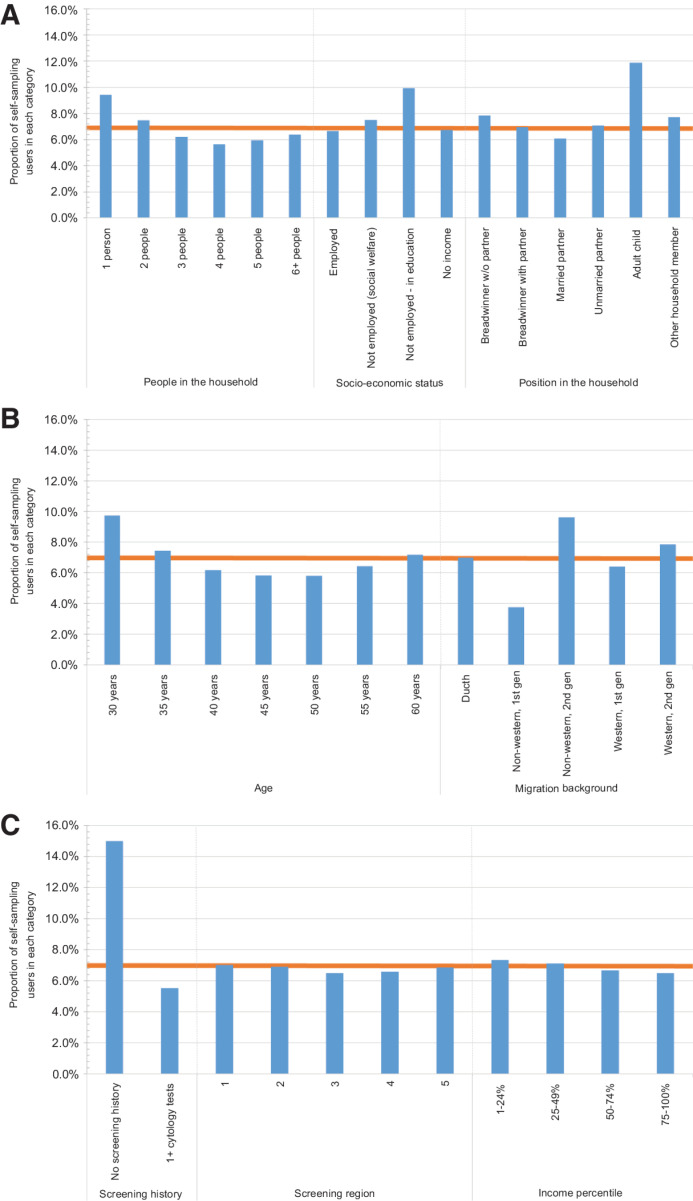
Results: Out of the 857,866 women, 6.8% chose to use a self-sampling device. A higher proportion of self-sampling users was ages 30 to 35 years, was not previously screened, was living in a one-person household, or was the breadwinner in the household. After adjustment for these factors self-sampling had lower hrHPV positivity (aOR, 0.65; 95% CI, 0.63-0.68)) as compared with clinician-collected sampling, as well as lower odds of CIN 2+ (aOR, 0.76; 95% CI, 0.70-0.82) and CIN 3+ (aOR, 0.86; 95% CI, 0.78-0.95) detection.
Conclusions: It is likely that the observed differences between the two sampling methods are not only related to sociodemographic differences, but related to differences in screening test accuracy and/or background risk.
Impact: Self-sampling can be used for targeting underscreened women, as a more convenient screening tool. Further investigation is required to evaluate how to implement self-sampling, when it is used as a primary instrument in routine screening. See related commentary by Arbyn et al., p. 159.
©2022 The Authors; Published by the American Association for Cancer Research.
Figures
Comment in
-
HPV-based Cervical Cancer Screening on Self-samples in the Netherlands: Challenges to Reach Women and Test Performance Questions.Cancer Epidemiol Biomarkers Prev. 2023 Feb 6;32(2):159-163. doi: 10.1158/1055-9965.EPI-22-1041. Cancer Epidemiol Biomarkers Prev. 2023. PMID: 36744312
References
-
- Bevolkingsonderzoek Nederland. De uitnodiging. c2020-21 [cited 26 July 2021]. Available from: https://www.bevolkingsonderzoeknederland.nl/baarmoederhalskanker/de-uitn....
-
- Rijksinstituut voor Volksgezondheid en Milieu (RIVM). Uitvoeringskader Bevolkingsonderzoek Baarmoederhalskanker. 2017[cited 26 July 2021]. Available from: https://www.rivm.nl/documenten/uitvoeringskader-bevolkingsonderzoek-baar....
-
- Polman NJ, de Haan Y, Veldhuijzen NJ, Heideman DAM, de Vet HCW, Meijer C, et al. Experience with HPV self-sampling and clinician-based sampling in women attending routine cervical screening in the Netherlands. Prev Med 2019;125:5–11. - PubMed
-
- Ketelaars PJW, Bosgraaf RP, Siebers AG, Massuger LFAG, van der Linden JC, Wauters CAP, et al. High-risk human papillomavirus detection in self-sampling compared to physician-taken smear in a responder population of the Dutch cervical screening: results of the VERA study. Preventive Medicine 2017;101:96–101. - PubMed
