

Reproductive outcome in 326 women with unicornuate uterus
- PMID: 36099518
- PMCID: PMC10107309
- DOI: 10.1002/uog.26073
Reproductive outcome in 326 women with unicornuate uterus
Abstract
Objectives: To study the reproductive outcomes of women with a unicornuate uterus and compare them to those of women with no congenital uterine anomaly.
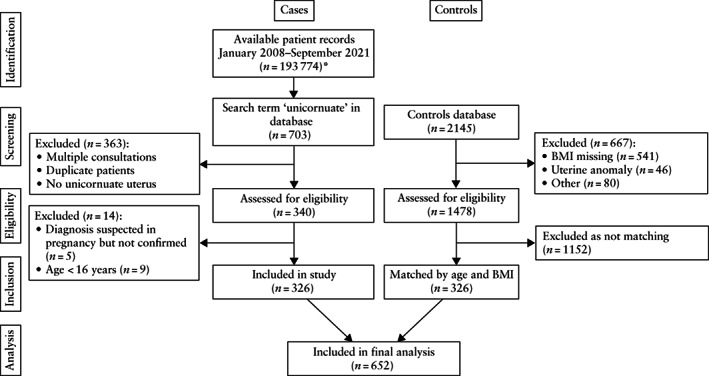
Methods: This was a single-center, retrospective cohort study. Cases were women aged at least 16 years who were diagnosed with a unicornuate uterus on transvaginal/transrectal ultrasound between January 2008 and September 2021. Controls were women with no congenital uterine anomaly matched 1:1 by age and body mass index. The primary outcome was live-birth rate. Secondary outcomes were pregnancy loss (miscarriage, ectopic pregnancy, termination of pregnancy), preterm delivery, mode of delivery and concomitant gynecological abnormalities (endometriosis, adenomyosis, fibroids).
Results: Included in the study were 326 cases and 326 controls. Women with a unicornuate uterus had a significantly lower live-birth rate (184/388 (47.4%) vs 229/396 (57.8%); P = 0.004) and higher rates of overall miscarriage (178/424 (42.0%) vs 155/465 (33.3%); adjusted odds ratio (aOR), 2.21 (95% CI, 1.42-3.42), P < 0.001), ectopic pregnancy (26/424 (6.1%) vs 11/465 (2.4%); aOR, 2.52 (95% CI, 1.22-5.22), P = 0.01), preterm delivery (45/184 (24.5%) vs 17/229 (7.4%); aOR, 3.04 (95% CI, 1.52-5.97), P = 0.001) and Cesarean delivery (116/184 (63.0%) vs 70/229 (30.6%); aOR, 2.54 (95% CI, 1.67-3.88), P < 0.001). Rudimentary-horn pregnancies accounted for 7/26 (26.9%) ectopic pregnancies in the study group. Women with a unicornuate uterus were more likely to have endometriosis (17.5% vs 10.7%; P = 0.018) and adenomyosis (26.7% vs 15.6%; P = 0.001), but were not more likely to have fibroids compared with controls. Women with a functional rudimentary horn were more likely to have pelvic endometriosis compared to those without (odds ratio, 2.4 (95% CI, 1.4-4.1), P = 0.002).
Conclusions: Pregnant women with a unicornuate uterus should be classified as high risk. Removal of a functional rudimentary horn should be discussed with the patient to prevent a rudimentary-horn ectopic pregnancy. © 2022 The Authors. Ultrasound in Obstetrics & Gynecology published by John Wiley & Sons Ltd on behalf of International Society of Ultrasound in Obstetrics and Gynecology.
Keywords: adenomyosis; ectopic pregnancy; endometriosis; miscarriage; uterine anomaly.
© 2022 The Authors. Ultrasound in Obstetrics & Gynecology published by John Wiley & Sons Ltd on behalf of International Society of Ultrasound in Obstetrics and Gynecology.
Figures
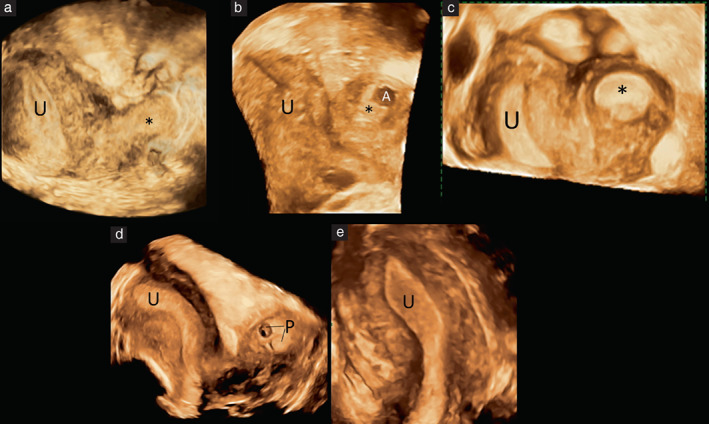
 ). (a) Right hemiuterus and non‐functional left rudimentary horn. Cavity of hemiuterus is narrow in fundal area and only a single interstitial portion of Fallopian tube is visible. (b) Right hemiuterus and non‐communicating left rudimentary horn. Cavity of horn contains functional endometrium with visible adenomyosis (A), represented by anechoic myometrial cyst with thin hyperechogenic rim protruding into cavity. (c) Right hemiuterus with hyperechogenic endometrium and functional, non‐communicating left rudimentary horn, with blood distending the cavity. (d) Right hemiuterus and duplex ectopic pregnancy in non‐communicating left rudimentary horn, where two gestational sacs (P) are visualized. (e) Right hemiuterus in same woman as in (d), 3 months after uneventful excision of rudimentary horn containing ectopic pregnancy.
). (a) Right hemiuterus and non‐functional left rudimentary horn. Cavity of hemiuterus is narrow in fundal area and only a single interstitial portion of Fallopian tube is visible. (b) Right hemiuterus and non‐communicating left rudimentary horn. Cavity of horn contains functional endometrium with visible adenomyosis (A), represented by anechoic myometrial cyst with thin hyperechogenic rim protruding into cavity. (c) Right hemiuterus with hyperechogenic endometrium and functional, non‐communicating left rudimentary horn, with blood distending the cavity. (d) Right hemiuterus and duplex ectopic pregnancy in non‐communicating left rudimentary horn, where two gestational sacs (P) are visualized. (e) Right hemiuterus in same woman as in (d), 3 months after uneventful excision of rudimentary horn containing ectopic pregnancy.
Similar articles
-
Obstetric outcomes of women with congenital uterine anomalies in the United States.Am J Obstet Gynecol MFM. 2024 Aug;6(8):101396. doi: 10.1016/j.ajogmf.2024.101396. Epub 2024 Jun 10. Am J Obstet Gynecol MFM. 2024. PMID: 38866133
-
Impact of congenital uterine anomalies on reproductive outcomes of IVF/ICSI-embryo transfer: a retrospective study.Eur J Med Res. 2024 Jan 11;29(1):48. doi: 10.1186/s40001-023-01544-2. Eur J Med Res. 2024. PMID: 38212852 Free PMC article.
-
The importance of the 'uterine factor' in recurrent pregnancy loss: a retrospective cohort study on women screened through 3D transvaginal ultrasound.Hum Reprod. 2024 Aug 1;39(8):1645-1655. doi: 10.1093/humrep/deae148. Hum Reprod. 2024. PMID: 38964365
-
The pregnancy outcomes of patients with rudimentary uterine horn: A 30-year experience.PLoS One. 2019 Jan 25;14(1):e0210788. doi: 10.1371/journal.pone.0210788. eCollection 2019. PLoS One. 2019. PMID: 30682068 Free PMC article. Review.
-
Pregnancy outcomes in unicornuate uteri: a review.Fertil Steril. 2009 May;91(5):1886-94. doi: 10.1016/j.fertnstert.2008.02.163. Epub 2008 Apr 25. Fertil Steril. 2009. PMID: 18439594 Review.
Cited by
-
Müllerian anomalies and endometriosis: associations and phenotypic variations.Reprod Biol Endocrinol. 2024 Dec 19;22(1):157. doi: 10.1186/s12958-024-01336-1. Reprod Biol Endocrinol. 2024. PMID: 39702195 Free PMC article. Review.
-
Ectopic pregnancy.Nat Rev Dis Primers. 2024 Dec 12;10(1):94. doi: 10.1038/s41572-024-00579-x. Nat Rev Dis Primers. 2024. PMID: 39668167 Review.
-
Successful pregnancy outcome via in-vitro fertilization and laparoscopic resection of non-communicating rudimentary horn pregnancy containing early pregnancy: a case report.BMC Pregnancy Childbirth. 2024 Feb 7;24(1):115. doi: 10.1186/s12884-024-06289-2. BMC Pregnancy Childbirth. 2024. PMID: 38326770 Free PMC article.
-
Neonates at Risk: Understanding the Impact of High-Risk Pregnancies on Neonatal Health.Medicina (Kaunas). 2025 Jun 11;61(6):1077. doi: 10.3390/medicina61061077. Medicina (Kaunas). 2025. PMID: 40572764 Free PMC article. Review.
-
Unicornuate Uterus with a Non-Communicating Rudimentary Horn: Challenges and Management of a Rare Pregnancy.Cureus. 2023 Jun 19;15(6):e40666. doi: 10.7759/cureus.40666. eCollection 2023 Jun. Cureus. 2023. PMID: 37485214 Free PMC article.
References
-
- Nahum GG. Uterine anomalies. How common are they, and what is their distribution among subtypes? J Reprod Med 1998; 43: 877–887. - PubMed
-
- Jurkovic D, Gruboeck K, Tailor A, Nicolaides KH. Ultrasound screening for congenital uterine anomalies. Br J Obstet Gynaecol 1997; 104: 1320–1321. - PubMed
-
- Prior M, Richardson A, Asif S, Polanski L, Parris‐Larkin M, Chandler J, Fogg L, Jassal P, Thornton JG, Raine‐Fenning NJ. Outcome of assisted reproduction in women with congenital uterine anomalies: a prospective observational study. Ultrasound Obstet Gynecol 2018; 51: 110–117. - PubMed
-
- Chan YY, Jayaprakasan K, Tan A, Thornton JG, Coomarasamy A, Raine‐Fenning NJ. Reproductive outcomes in women with congenital uterine anomalies: a systematic review. Ultrasound Obstet Gynecol 2011; 38: 371–382. - PubMed
-
- Fedele L, Bianchi S, Agnoli B, Tozzi L, Vignali M. Urinary tract anomalies associated with unicornuate uterus. J Urol 1996; 155: 847–848. - PubMed
