

Fluorescent Indocyanine Green versus Technetium-99m and Blue Dye for Bilateral SENTinel Lymph Node Detection in Stage I-IIA Cervical Cancer (FluoreSENT): protocol for a non-inferiority study
- PMID: 36100304
- PMCID: PMC9472172
- DOI: 10.1136/bmjopen-2022-061829
Fluorescent Indocyanine Green versus Technetium-99m and Blue Dye for Bilateral SENTinel Lymph Node Detection in Stage I-IIA Cervical Cancer (FluoreSENT): protocol for a non-inferiority study
Abstract
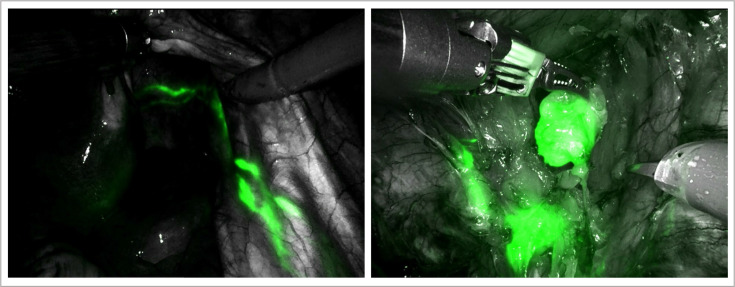
Introduction: Nowadays, two predominant methods for detecting sentinel lymph nodes (SLNs) in cervical cancer are in use. The most conventional method is a combination of a radiotracer, technetium-99m (99mTc) and blue dye. More recently, another method for SLN mapping using indocyanine green (ICG) is becoming widely accepted. ICG is a fluorescent dye, visualised intraoperatively with near-infrared (NIR) fluorescence imaging, providing real-time visual navigation. The presumed advantages of ICG over 99mTc, that is, being cheaper, non-radioactive and logistically more attractive, are only valuable if its detection rate proves to be at least non-inferior. Before omitting the well-functioning and evidence-based combined approach of 99mTc and blue dye, we aim to provide prospective evidence on the non-inferiority of ICG with NIR fluorescence imaging.
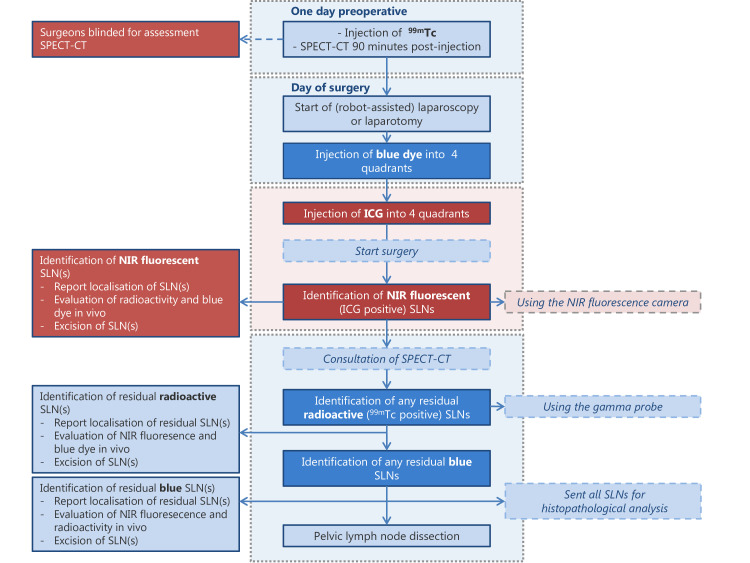
Methods and analysis: We initiated a prospective non-inferiority study with a paired comparison of both SLN methods in a single sample of 101 patients with International Federation of Gynecology and Obstetrics (FIGO) stage IA-IB2 or IIA1 cervical cancer receiving primary surgical treatment. All patients undergo SLN mapping with ICG and NIR fluorescence imaging in adjunct to mapping with 99mTc (including single photon emission computed tomography with X-ray computed tomography (SPECT/CT)) and blue dye. Surgeons start SLN detection with ICG while being blinded for the preoperative outcome of SPECT/CT to avoid biased detection with ICG. Primary endpoint of this study is bilateral SLN detection rate of both methods (ie, detection of at least one SLN in each hemipelvis). Since we compare strategies for SLN mapping that are already applied in current daily practice for different types of cancer, no additional risks or burdens are expected from these study procedures.
Ethics and dissemination: The current study is approved by the Medical Ethics Research Committee Utrecht (reference number 21-014). Findings arising from this study will be disseminated in peer-reviewed journals, academic conferences and through patient organisations.
Trial registration number: NL9011 and EudraCT 2020-005134-15.
Keywords: Diagnostic radiology; GYNAECOLOGY; Gynaecological oncology; Nuclear radiology; ONCOLOGY.
© Author(s) (or their employer(s)) 2022. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: RPZ is a proctor for robot-assisted surgery in gynaecological oncology on behalf of Intuitive Surgical.
Figures
Similar articles
-
Impact of Indocyanine Green for Sentinel Lymph Node Mapping in Early Stage Endometrial and Cervical Cancer: Comparison with Conventional Radiotracer (99m)Tc and/or Blue Dye.Ann Surg Oncol. 2016 Jul;23(7):2183-91. doi: 10.1245/s10434-015-5022-1. Epub 2015 Dec 29. Ann Surg Oncol. 2016. PMID: 26714944 Free PMC article.
-
Combining Indocyanine Green and Tc99-nanocolloid does not increase the detection rate of sentinel lymph nodes in early stage cervical cancer compared to Indocyanine Green alone.Gynecol Oncol. 2020 Feb;156(2):335-340. doi: 10.1016/j.ygyno.2019.11.026. Epub 2019 Nov 26. Gynecol Oncol. 2020. PMID: 31780237
-
Comparison of SPECT-CT with intraoperative mapping in cervical and uterine malignancies.Int J Gynecol Cancer. 2021 May;31(5):679-685. doi: 10.1136/ijgc-2020-002198. Epub 2021 Mar 1. Int J Gynecol Cancer. 2021. PMID: 33649157
-
Sentinel node biopsy for diagnosis of lymph node involvement in endometrial cancer.Cochrane Database Syst Rev. 2021 Jun 9;6(6):CD013021. doi: 10.1002/14651858.CD013021.pub2. Cochrane Database Syst Rev. 2021. PMID: 34106467 Free PMC article.
-
Indocyanine green versus technetium-99m with blue dye for sentinel lymph node detection in early-stage cervical cancer: A systematic review and meta-analysis.Cancer Rep (Hoboken). 2022 Jan;5(1):e1401. doi: 10.1002/cnr2.1401. Epub 2021 May 11. Cancer Rep (Hoboken). 2022. PMID: 33973745 Free PMC article.
Cited by
-
Application of fluorescence endoscopy with methylene blue dye and indocyanine green dual-tracer method in sentinel lymph node biopsy for women with breast cancer.Gland Surg. 2023 Jun 30;12(6):780-790. doi: 10.21037/gs-22-469. Epub 2023 Jun 12. Gland Surg. 2023. PMID: 37441014 Free PMC article.