

Hospital Variation in Preference for a Specific Bariatric Procedure and the Association with Weight Loss Performance: a Nationwide Analysis
- PMID: 36100807
- PMCID: PMC9613549
- DOI: 10.1007/s11695-022-06212-8
Hospital Variation in Preference for a Specific Bariatric Procedure and the Association with Weight Loss Performance: a Nationwide Analysis
Abstract
Purpose: Hospitals performing a certain bariatric procedure in high volumes may have better outcomes. However, they could also have worse outcomes for some patients who are better off receiving another procedure. This study evaluates the effect of hospital preference for a specific type of bariatric procedure on their overall weight loss results.
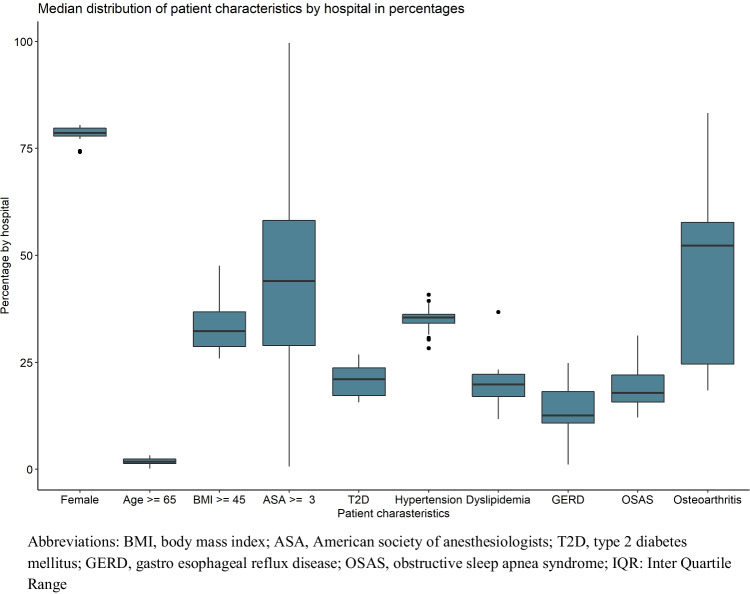
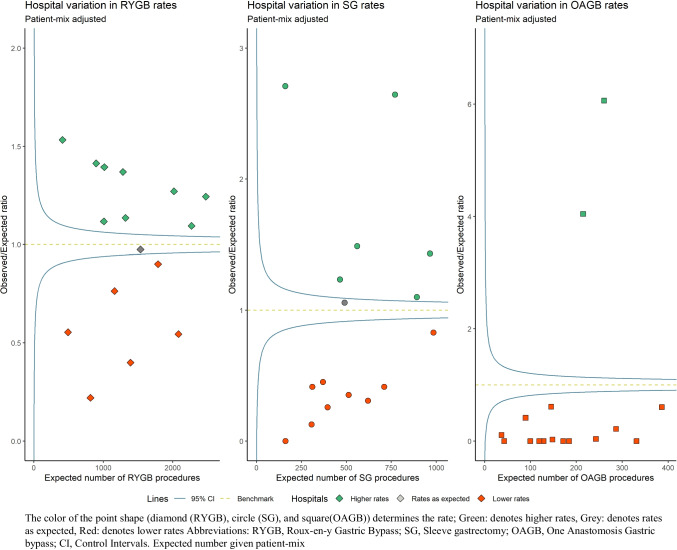
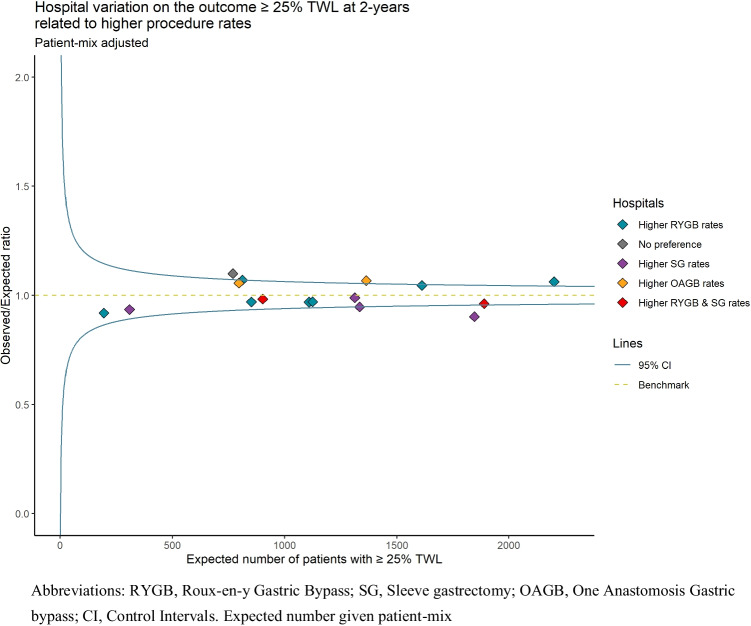
Methods: All hospitals performing bariatric surgery were included from the nationwide Dutch Audit for Treatment of Obesity. For each hospital, the expected (E) numbers of sleeve gastrectomy (SG), Roux-en-Y gastric bypass (RYGB), and one-anastomosis gastric bypass (OAGB) were calculated given their patient-mix. These were compared with the observed (O) numbers as the O/E ratio in a funnel plot. The 95% control intervals were used to identify outlier hospitals performing a certain procedure significantly more often than expected given their patient-mix (defined as hospital preference for that procedure). Similarly, funnel plots were created for the outcome of patients achieving ≥ 25% total weight loss (TWL) after 2 years, which was linked to each hospital's preference.
Results: A total of 34,558 patients were included, with 23,154 patients completing a 2-year follow-up, of whom 79.6% achieved ≥ 25%TWL. Nine hospitals had a preference for RYGB (range O/E ratio [1.09-1.53]), with 1 having significantly more patients achieving ≥ 25%TWL (O/E ratio [1.06]). Of 6 hospitals with a preference for SG (range O/E ratio [1.10-2.71]), one hospital had significantly fewer patients achieving ≥ 25%TWL (O/E ratio [0.90]), and from two hospitals with a preference for OAGB (range O/E ratio [4.0-6.0]), one had significantly more patients achieving ≥ 25%TWL (O/E ratio [1.07]). One hospital had no preference for any procedure but did have significantly more patients achieving ≥ 25%TWL (O/E ratio [1.10]).
Conclusion: Hospital preference is not consistently associated with better overall weight loss results. This suggests that even though experience with a procedure may be slightly less in hospitals not having a preference, it is still sufficient to achieve similar weight loss outcomes when surgery is provided in centralized high-volume bariatric institutions.
Keywords: Bariatric surgery; Centralized bariatric care; Hospital preference; Hospital variation; Hospital volume; Textbook outcome; Weight loss.
© 2022. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Musella M, Vitiello A. The YOMEGA non-inferiority trial. Lancet. Elsevier; 2019;394:1412. - PubMed
-
- O’Brien P, Hindle A, Brennan L, et al. Long-term outcomes after bariatric surgery: a systematic review and meta-analysis of weight loss at 10 or more years for all bariatric procedures and a single-centre review of 20-year outcomes after adjustable gastric banding. Obes Surg. 2019;29:3–14. doi: 10.1007/s11695-018-3525-0. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
