

Respiratory support in patients with severe COVID-19 in the International Severe Acute Respiratory and Emerging Infection (ISARIC) COVID-19 study: a prospective, multinational, observational study
- PMID: 36100904
- PMCID: PMC9469080
- DOI: 10.1186/s13054-022-04155-1
Respiratory support in patients with severe COVID-19 in the International Severe Acute Respiratory and Emerging Infection (ISARIC) COVID-19 study: a prospective, multinational, observational study
Abstract
Background: Up to 30% of hospitalised patients with COVID-19 require advanced respiratory support, including high-flow nasal cannulas (HFNC), non-invasive mechanical ventilation (NIV), or invasive mechanical ventilation (IMV). We aimed to describe the clinical characteristics, outcomes and risk factors for failing non-invasive respiratory support in patients treated with severe COVID-19 during the first two years of the pandemic in high-income countries (HICs) and low middle-income countries (LMICs).
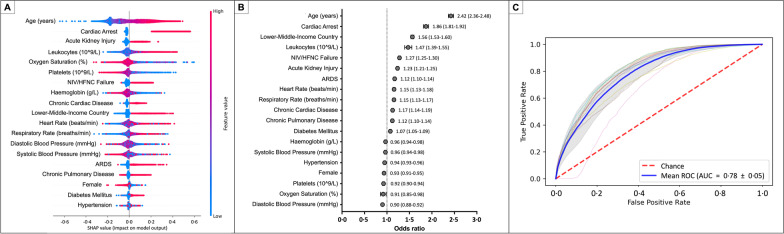
Methods: This is a multinational, multicentre, prospective cohort study embedded in the ISARIC-WHO COVID-19 Clinical Characterisation Protocol. Patients with laboratory-confirmed SARS-CoV-2 infection who required hospital admission were recruited prospectively. Patients treated with HFNC, NIV, or IMV within the first 24 h of hospital admission were included in this study. Descriptive statistics, random forest, and logistic regression analyses were used to describe clinical characteristics and compare clinical outcomes among patients treated with the different types of advanced respiratory support.
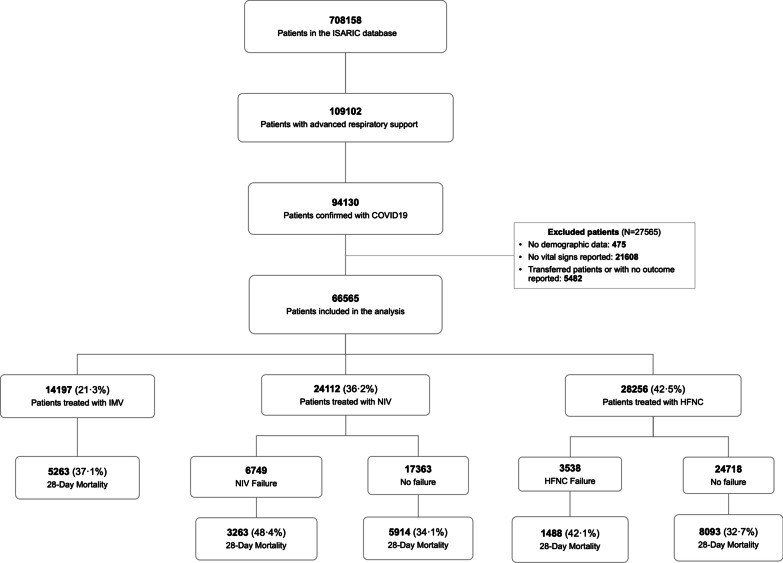
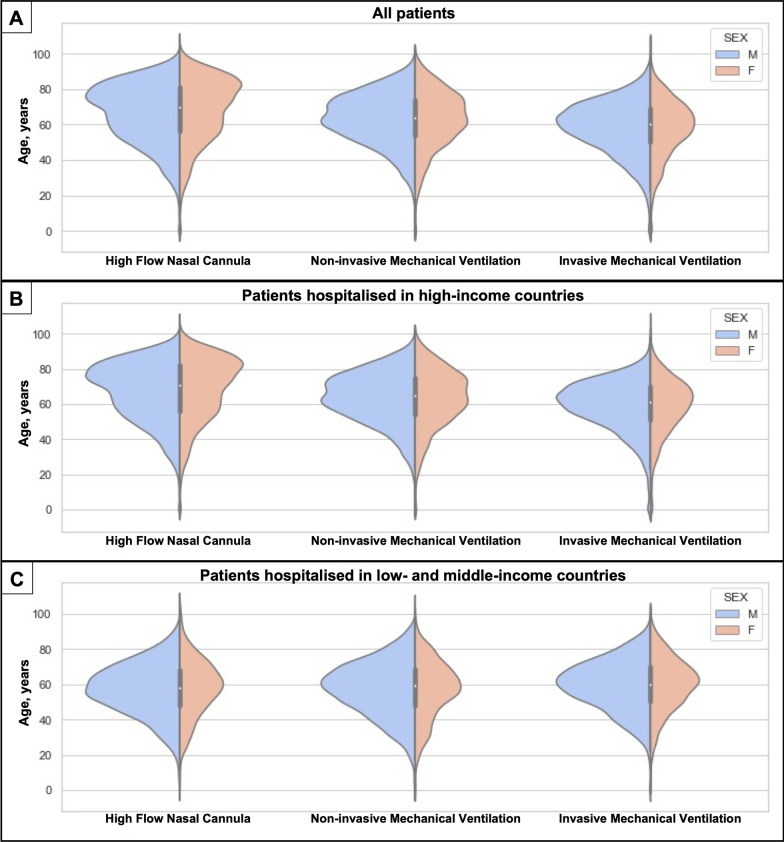
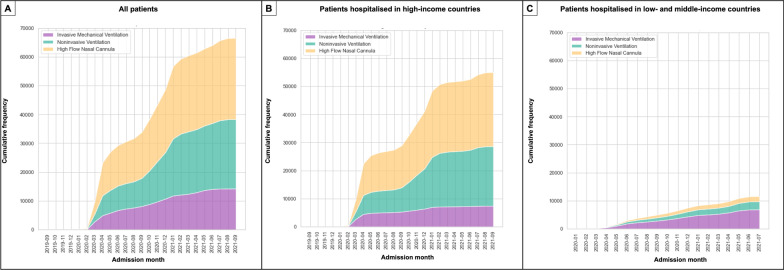
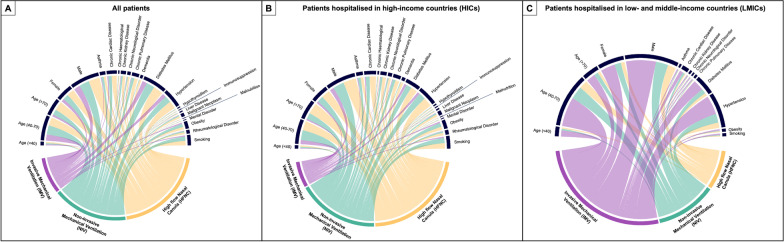
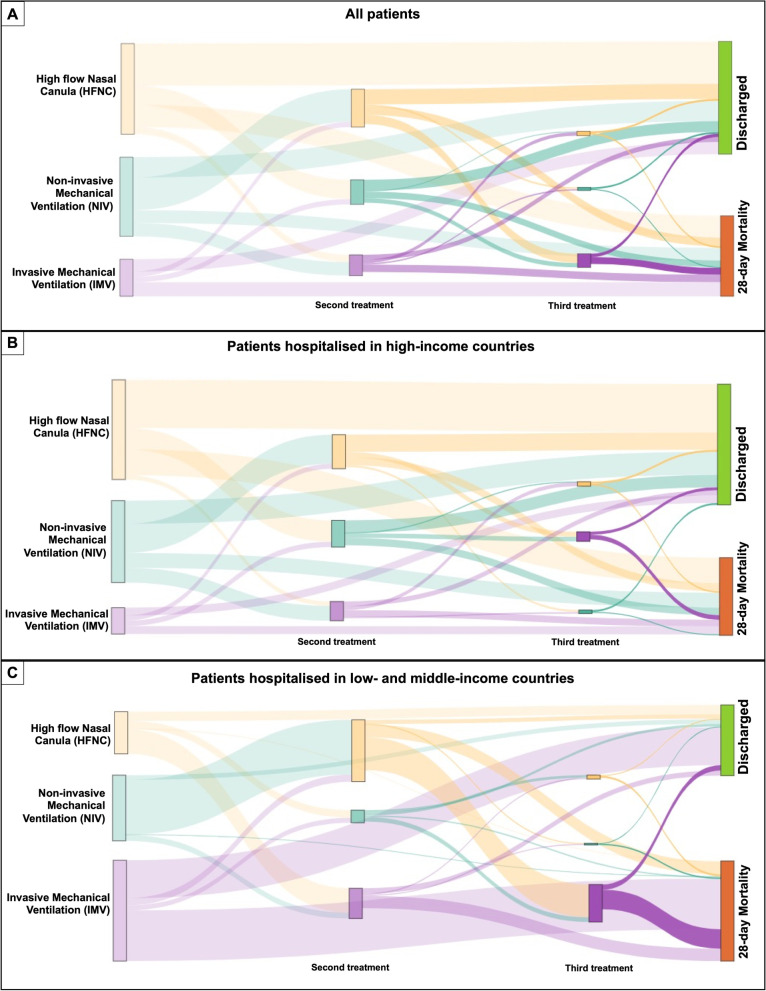
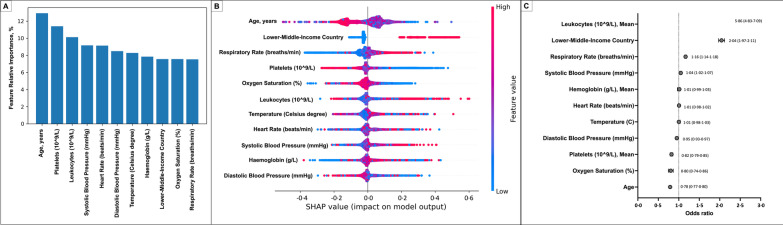
Results: A total of 66,565 patients were included in this study. Overall, 82.6% of patients were treated in HIC, and 40.6% were admitted to the hospital during the first pandemic wave. During the first 24 h after hospital admission, patients in HICs were more frequently treated with HFNC (48.0%), followed by NIV (38.6%) and IMV (13.4%). In contrast, patients admitted in lower- and middle-income countries (LMICs) were less frequently treated with HFNC (16.1%) and the majority received IMV (59.1%). The failure rate of non-invasive respiratory support (i.e. HFNC or NIV) was 15.5%, of which 71.2% were from HIC and 28.8% from LMIC. The variables most strongly associated with non-invasive ventilation failure, defined as progression to IMV, were high leukocyte counts at hospital admission (OR [95%CI]; 5.86 [4.83-7.10]), treatment in an LMIC (OR [95%CI]; 2.04 [1.97-2.11]), and tachypnoea at hospital admission (OR [95%CI]; 1.16 [1.14-1.18]). Patients who failed HFNC/NIV had a higher 28-day fatality ratio (OR [95%CI]; 1.27 [1.25-1.30]).
Conclusions: In the present international cohort, the most frequently used advanced respiratory support was the HFNC. However, IMV was used more often in LMIC. Higher leucocyte count, tachypnoea, and treatment in LMIC were risk factors for HFNC/NIV failure. HFNC/NIV failure was related to worse clinical outcomes, such as 28-day mortality. Trial registration This is a prospective observational study; therefore, no health care interventions were applied to participants, and trial registration is not applicable.
Keywords: COVID-19; Critical care; High flow nasal cannula; Invasive mechanical ventilation.
© 2022. The Author(s).
Conflict of interest statement
See Additional file 2.
Figures
References
-
- Reyes LF, Murthy S, Garcia-Gallo E, Irvine M, Merson L, Martin-Loeches I, Rello J, Taccone FS, Fowler RA, Docherty AB, et al. Clinical characteristics, risk factors and outcomes in patients with severe COVID-19 registered in the International Severe Acute Respiratory and Emerging Infection Consortium WHO clinical characterisation protocol: a prospective, multinational, multicentre, observational study. ERJ Open Res. 2022;8(1):66. doi: 10.1183/23120541.00552-2021. - DOI - PMC - PubMed
-
- Knight SR, Ho A, Pius R, Buchan I, Carson G, Drake TM, Dunning J, Fairfield CJ, Gamble C, Green CA, et al. Risk stratification of patients admitted to hospital with covid-19 using the ISARIC WHO Clinical Characterisation Protocol: development and validation of the 4C Mortality Score. BMJ. 2020;370:m3339. doi: 10.1136/bmj.m3339. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
- OV2170359/CIHR Coronavirus Rapid Research Funding Opportunity
- H2020 project 101003589/Grants from Rapid European COVID-19 Emergency Response research (RECOVER)
- MC_PC_19059/MRC_/Medical Research Council/United Kingdom
- WT_/Wellcome Trust/United Kingdom
- MR/S032304/1/MRC_/Medical Research Council/United Kingdom
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
