

Sex Differences in Subclinical Atherosclerosis and Systemic Immune Activation/Inflammation Among People With Human Immunodeficiency Virus in the United States
- PMID: 36101518
- PMCID: PMC9839188
- DOI: 10.1093/cid/ciac767
Sex Differences in Subclinical Atherosclerosis and Systemic Immune Activation/Inflammation Among People With Human Immunodeficiency Virus in the United States
Abstract
Background: Among people with HIV (PWH), sex differences in presentations of atherosclerotic cardiovascular disease (ASCVD) may be influenced by differences in coronary plaque parameters, immune/inflammatory biomarkers, or relationships therein.
Methods: REPRIEVE, a primary ASCVD prevention trial, enrolled antiretroviral therapy (ART)-treated PWH. At entry, a subset of US participants underwent coronary computed tomography angiography (CTA) and immune phenotyping (n = 755 CTA; n = 725 CTA + immune). We characterized sex differences in coronary plaque and immune/inflammatory biomarkers and compared immune-plaque relationships by sex. Unless noted otherwise, analyses adjust for ASCVD risk score.
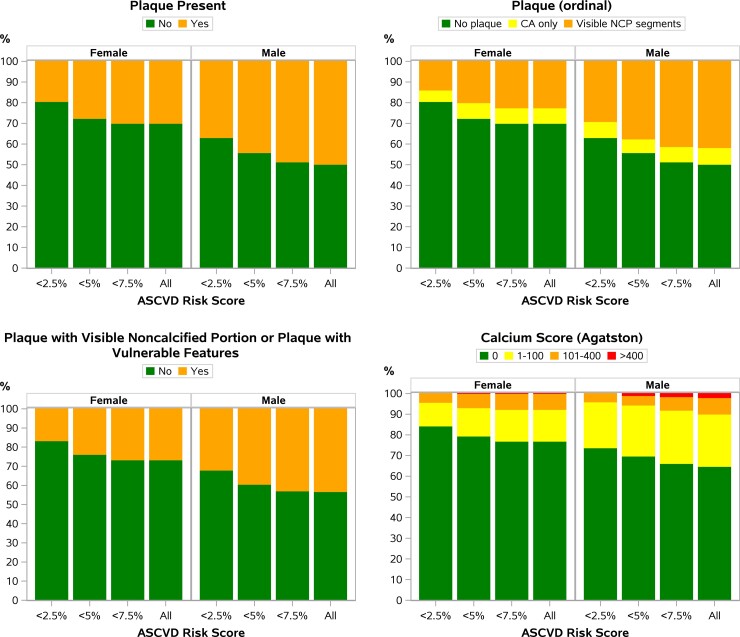
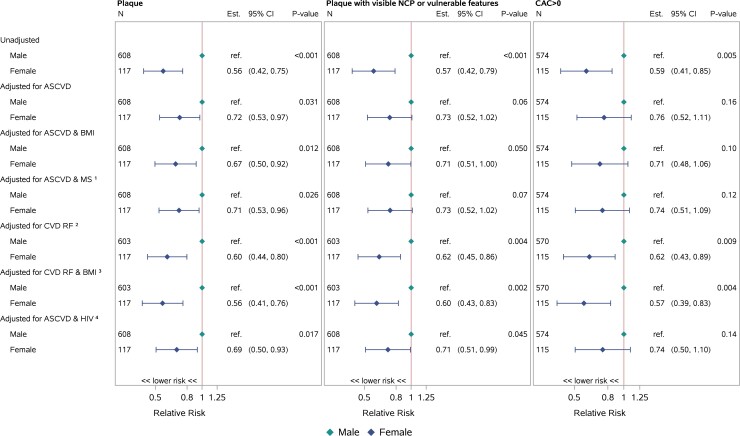
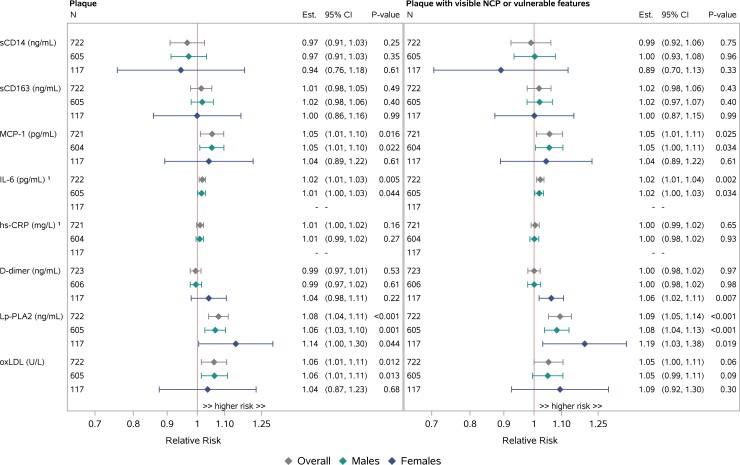
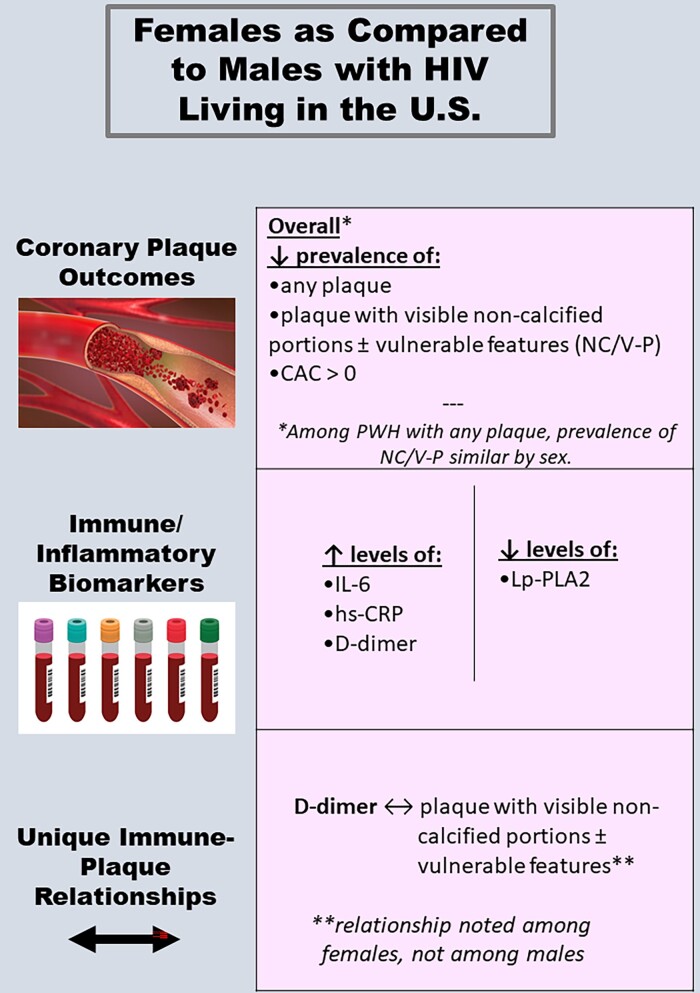
Results: The primary analysis cohort included 631 males and 124 females. ASCVD risk was higher among males (median: 4.9% vs 2.1%), while obesity rates were higher among females (48% vs 21%). Prevalence of any plaque and of plaque with either ≥1 visible noncalcified portion or vulnerable features (NC/V-P) was lower among females overall and controlling for relevant risk factors (RR [95% CI] for any plaque: .67 [.50, .92]; RR for NC/V-P: .71 [.51, 1.00] [adjusted for ASCVD risk score and body mass index]). Females showed higher levels of IL-6, hs-CRP, and D-dimer and lower levels of Lp-PLA2 (P < .001 for all). Higher levels of Lp-PLA2, MCP-1, and oxLDL were associated with higher plaque (P < .02) and NC/V-P prevalence, with no differences by sex. Among females but not males, D-dimer was associated with higher prevalence of NC/V-P (interaction P = .055).
Conclusions: Among US PWH, females had a lower prevalence of plaque and NC/V-P, as well as differences in key immune/inflammatory biomarkers. Immune-plaque relationships differed by sex for D-dimer but not other tested parameters. Clinical Trial Registration. ClinicalTrials.gov; identifier: NCT0234429 (date of initial registration: 22 January 2015).
Trial registration: ClinicalTrials.gov NCT00234429.
Keywords: HIV; coronary atherosclerosis; inflammation; reproductive aging; women.
© The Author(s) 2022. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Figures
References
-
- Schnittman S, Beck-Engeser G, Shigenaga J, Ahn H, et al. . Sex modifies the association between inflammation and vascular events in treated HIV. Presented at: Conference on Retroviruses and Opportunistic Infection; 6–10 March 2021; Virtual. Abstract 98.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- UM1 AI069494/AI/NIAID NIH HHS/United States
- UM1 AI069501/AI/NIAID NIH HHS/United States
- UM1 AI069432/AI/NIAID NIH HHS/United States
- UM1 AI069471/AI/NIAID NIH HHS/United States
- R01 AG054366/AG/NIA NIH HHS/United States
- UM1 AI068634/AI/NIAID NIH HHS/United States
- K24 AI157882/AI/NIAID NIH HHS/United States
- UL1 TR002384/TR/NCATS NIH HHS/United States
- U01 AI069424/AI/NIAID NIH HHS/United States
- U01 HL123336/HL/NHLBI NIH HHS/United States
- UM1 AI069419/AI/NIAID NIH HHS/United States
- P30 DK048520/DK/NIDDK NIH HHS/United States
- UM1 AI069424/AI/NIAID NIH HHS/United States
- UM1 AI068636/AI/NIAID NIH HHS/United States
- P30 AI050410/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
