

Predicting Time to Death After Withdrawal of Life-Sustaining Treatment in Children
- PMID: 36101830
- PMCID: PMC9462532
- DOI: 10.1097/CCE.0000000000000764
Predicting Time to Death After Withdrawal of Life-Sustaining Treatment in Children
Abstract
Accurately predicting time to death after withdrawal of life-sustaining treatment is valuable for family counseling and for identifying candidates for organ donation after cardiac death. This topic has been well studied in adults, but literature is scant in pediatrics. The purpose of this report is to assess the performance and clinical utility of the available tools for predicting time to death after treatment withdrawal in children.
Data sources: Terms related to predicting time to death after treatment withdrawal were searched in PubMed and Embase from 1993 to November 2021.
Study selection: Studies endeavoring to predict time to death or describe factors related to time to death were included. Articles focusing on perceptions or practices of treatment withdrawal were excluded.
Data extraction: Titles, abstracts, and full text of articles were screened to determine eligibility. Data extraction was performed manually. Two-by-two tables were reconstructed with available data from each article to compare performance metrics head to head.
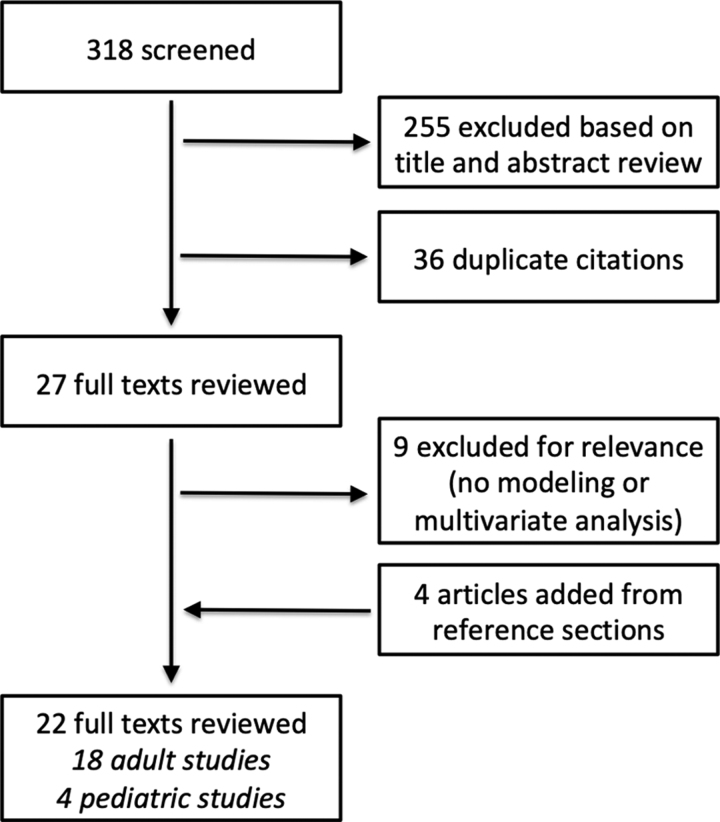
Data synthesis: Three hundred eighteen citations were identified from the initial search, resulting in 22 studies that were retained for full-text review. Among the pediatric studies, predictive models were developed using multiple logistic regression, Cox proportional hazards, and an advanced machine learning algorithm. In each of the original model derivation studies, the models demonstrated a classification accuracy ranging from 75% to 91% and positive predictive value ranging from 0.76 to 0.93.
Conclusions: There are few tools to predict time to death after withdrawal of life-sustaining treatment in children. They are limited by small numbers and incomplete validation. Future work includes utilization of advanced machine learning models.
Keywords: decision support techniques; intensive care units; machine learning; pediatric; terminal care; tissue and organ procurement.
Copyright © 2022 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of the Society of Critical Care Medicine.
Conflict of interest statement
Supported, in part, by the LK Whittier Foundation. The authors have disclosed that they do not have any potential conflicts of interest.
References
-
- Meert KL, Keele L, Morrison W, et al. ; Eunice Kennedy Shriver National Institute of Child Health and Human Development Collaborative Pediatric Critical Care Research Network: End-of-life practices among tertiary care PICUs in the United States: A multicenter study. Pediatr Crit Care Med 2015; 16:e231–e238 - PMC - PubMed
-
- Sands R, Manning JC, Vyas H, et al. : Characteristics of deaths in paediatric intensive care: A 10-year study. Nurs Crit Care 2009; 14:235–240 - PubMed
-
- Munshi L, Dhanani S, Shemie SD, et al. : Predicting time to death after withdrawal of life-sustaining therapy. Intensive Care Med 2015; 41:1014–1028 - PubMed
-
- Kotsopoulos AMM, Böing-Messing F, Jansen NE, et al. : External validation of prediction models for time to death in potential donors after circulatory death. Am J Transplant 2018; 18:890–896 - PubMed
-
- de Groot YJ, Lingsma HF, Bakker J, et al. : External validation of a prognostic model predicting time of death after withdrawal of life support in neurocritical patients. Crit Care Med 2012; 40:233–238 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
