

Safety and Efficacy of Pediatric Growth Hormone Therapy: Results From the Full KIGS Cohort
- PMID: 36102184
- PMCID: PMC9693805
- DOI: 10.1210/clinem/dgac517
Safety and Efficacy of Pediatric Growth Hormone Therapy: Results From the Full KIGS Cohort
Abstract
Context: The Kabi/Pfizer International Growth Database (KIGS) is a large, international database (1987-2012) of children treated with recombinant human growth hormone (rhGH) in real-world settings.
Objective: This work aimed to evaluate the safety and efficacy of rhGH from the full KIGS cohort.
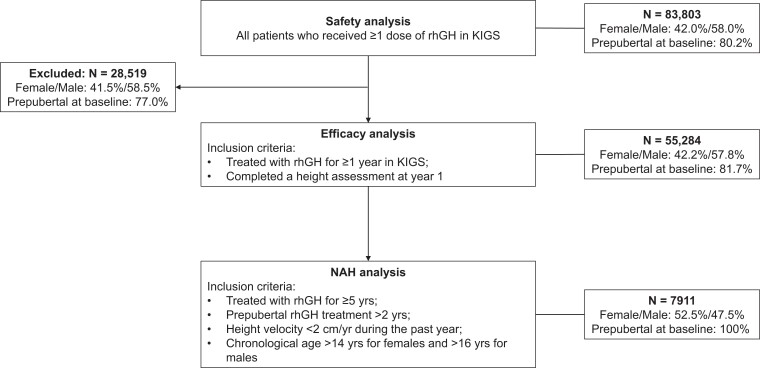
Methods: Data were collected by investigators from children with growth disorders treated with rhGH (Genotropin [somatropin]; Pfizer). Safety was evaluated in all treated patients, and efficacy in those treated for 1 year or more. A subgroup included patients treated for 5 years or more (≥ 2 years prepubertal) who had reached near-adult height (NAH). Main outcomes included adverse events (AEs), serious AEs (SAEs), and height growth.
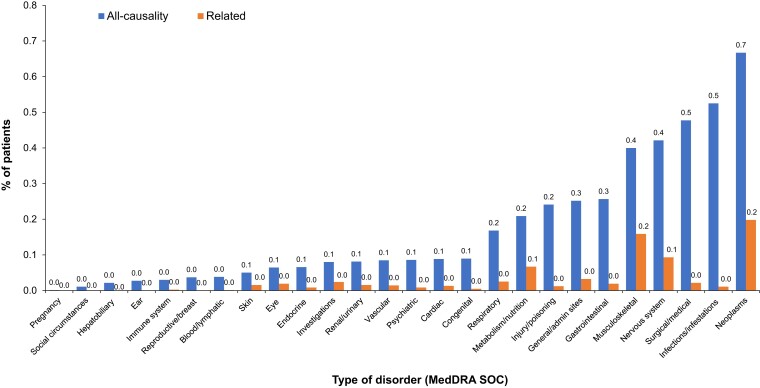
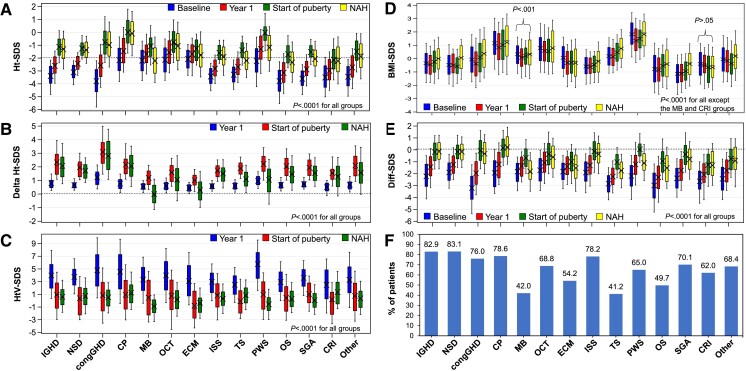
Results: The full KIGS cohort (N = 83 803 [58% male]) was treated for idiopathic GH deficiency (IGHD; 46.9%), organic GHD (10.0%), small for gestational age (SGA; 9.5%), Turner syndrome (TS; 9.2%), idiopathic short stature (ISS; 8.2%), and others (16.2%). Median rhGH treatment duration was 2.7 years and observation 3.1 years. SAEs occurred in 3.7% of patients and death in 0.4%. The most common SAEs were recurrence of craniopharyngioma (n = 151), neoplasm (n = 99), and cancer (n = 91); and scoliosis (n = 91). Median first-year delta height-SD score (SDS) (Prader) in prepubertal patients was 0.66 (IGHD), 0.55 (ISS), 0.58 (TS), and 0.71 (SGA). Median gains in NAH-SDS were 1.79 (IGHD), 1.37 (ISS), and 1.34 (SGA) for boys, and 2.07 (IGHD), 1.62 (ISS), 1.07 (TS), and 1.57 (SGA) for girls.
Conclusion: Data from KIGS, the largest and longest running international database of rhGH-treated children, show that rhGH is safe and increases short-term height gain and adult height across GHD and non-GHD conditions.
Keywords: KIGS; children; efficacy; growth hormone; safety; short stature.
© The Author(s) 2022. Published by Oxford University Press on behalf of the Endocrine Society.
Figures
Comment in
-
From the Full KIGS Cohort: On Safety and Efficacy of Growth Hormone Treatment.J Clin Endocrinol Metab. 2022 Dec 17;108(1):e1-e2. doi: 10.1210/clinem/dgac625. J Clin Endocrinol Metab. 2022. PMID: 36285732 No abstract available.
-
Letter to the Editor From Virú-Loza and Chávez-Nomberto: "Safety and Efficacy of Pediatric Growth Hormone Therapy: Results From the Full KIGS Cohort".J Clin Endocrinol Metab. 2023 May 17;108(6):e354-e355. doi: 10.1210/clinem/dgad054. J Clin Endocrinol Metab. 2023. PMID: 36719012 No abstract available.
-
Response to Letter to the Editor From Virú-Loza and Chávez-Nomberto: "Safety and Efficacy of Pediatric Growth Hormone Therapy: Results From the Full KIGS Cohort".J Clin Endocrinol Metab. 2023 May 17;108(6):e356-e357. doi: 10.1210/clinem/dgad055. J Clin Endocrinol Metab. 2023. PMID: 36721915 Free PMC article. No abstract available.
References
-
- Raben MS. Treatment of a pituitary dwarf with human growth hormone. J Clin Endocrinol Metab. 1958;18(8):901–903. - PubMed
-
- Ranke MB, Wit JM. Growth hormone—past, present and future. Nat Rev Endocrinol. 2018;14(5):285–300. - PubMed
-
- van Santen HM. Safety of GH after treatment for childhood cancer. Eur J Endocrinol. 2020;183(6):C15–C18. - PubMed
