

Comparative effectiveness of guselkumab in psoriatic arthritis: updates to a systematic literature review and network meta-analysis
- PMID: 36102818
- PMCID: PMC10070072
- DOI: 10.1093/rheumatology/keac500
Comparative effectiveness of guselkumab in psoriatic arthritis: updates to a systematic literature review and network meta-analysis
Abstract
Objective: The IL-23 p19-subunit inhibitor guselkumab has been previously compared with other targeted therapies for PsA through network meta-analysis (NMA). The objective of this NMA update was to include new guselkumab COSMOS trial data, and two key comparators: the IL-23 inhibitor risankizumab and the Janus kinase (JAK) inhibitor upadacitinib.
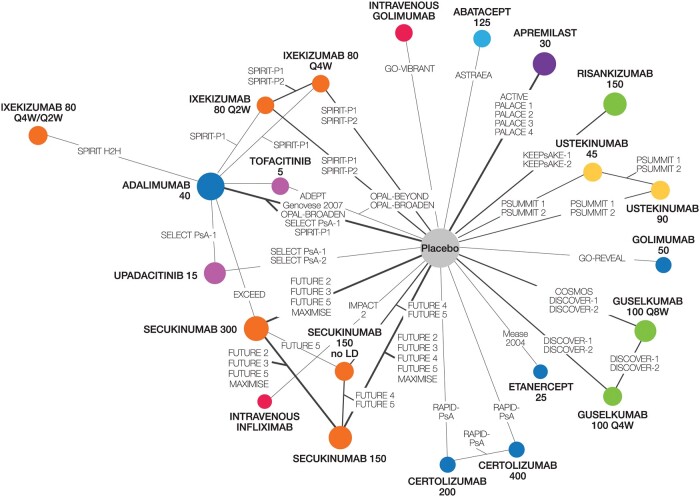
Material and methods: A systematic literature review was conducted to identify randomized controlled trials up to February 2021. A hand-search identified newer agents up to July 2021. Bayesian NMAs were performed to compare treatments on ACR response, Psoriasis Area and Severity Index (PASI) response, modified van der Heijde-Sharp (vdH-S) score, and serious adverse events (SAEs).
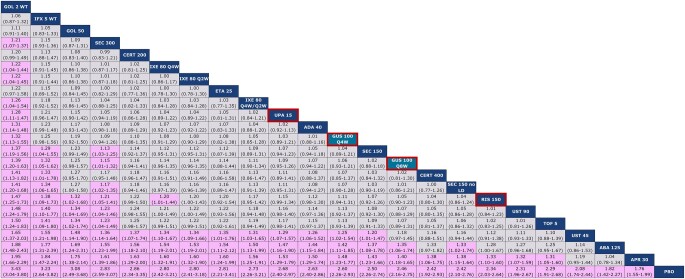
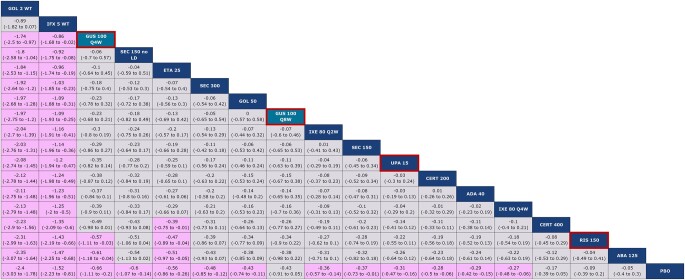
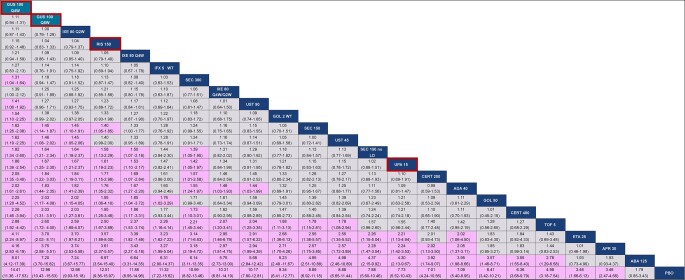
Results: For ACR 20, guselkumab 100 mg every 8 weeks (Q8W) and every 4 weeks (Q4W) were comparable (i.e. overlap in credible intervals) to most other agents, including risankizumab, upadacitinib, subcutaneous TNF inhibitors and most IL-17A inhibitors. For PASI 90, guselkumab Q8W and Q4W were better than multiple agents, including subcutaneous TNF and JAK inhibitors. For vdH-S, guselkumab Q8W was similar to risankizumab, while guselkumab Q4W was better; both doses were comparable to most other agents. Most agents had comparable SAEs.
Conclusions: Guselkumab demonstrates better skin efficacy than most other targeted PsA therapies, including upadacitinib. For vdH-S, both guselkumab doses are comparable to most treatments, with both doses ranking higher than most, including upadacitinib and risankizumab. Both guselkumab doses demonstrate comparable ACR responses to most other agents, including upadacitinib and risankizumab, and rank favourably in the network for SAEs.
Keywords: ACR response; Comparative effectiveness research; PsA; Psoriasis Area and Severity Index (PASI) response; guselkumab; modified van der Heijde–Sharp (vdH-S) score; network meta-analysis; serious adverse events; systematic literature review.
© The Author(s) 2022. Published by Oxford University Press on behalf of the British Society for Rheumatology.
Figures


References
-
- Wervers K, Luime JJ, Tchetverikov I. et al. Influence of disease manifestations on health-related quality of life in early psoriatic arthritis. J Rheumatol 2018;45:1526–31. - PubMed
-
- McInnes IB, Behrens F, Mease PJ. et al.; EXCEED Study Group. Secukinumab versus adalimumab for treatment of active psoriatic arthritis (EXCEED): a double-blind, parallel-group, randomised, active-controlled, phase 3b trial. Lancet 2020;395:1496–505. - PubMed
-
- Mease PJ, Smolen JS, Behrens F. et al.; SPIRIT H2H study group. A head-to-head comparison of the efficacy and safety of ixekizumab and adalimumab in biological-naïve patients with active psoriatic arthritis: 24-week results of a randomized, open-label, blinded-assessor trial. Ann Rheum Dis 2020;79:123–31. - PMC - PubMed
-
- Marzo-Ortega H, Packham J, Pujades-Rodriguez M.. ‘Too much of a good thing’: can network meta-analysis guide treatment decision-making in psoriatic arthritis? Rheumatology (Oxford) 2021;60:3042–4. - PubMed
-
- Catalá-López F, Tobías A, Cameron C, Moher D, Hutton B.. Network meta-analysis for comparing treatment effects of multiple interventions: an introduction. Rheumatol Int 2014;34:1489–96. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
