

Pattern of lymph node metastases in gastric cancer: a side-study of the multicenter LOGICA-trial
- PMID: 36103060
- PMCID: PMC9587950
- DOI: 10.1007/s10120-022-01329-2
Pattern of lymph node metastases in gastric cancer: a side-study of the multicenter LOGICA-trial
Abstract
Background: The relation between gastric cancer characteristics and lymph node (LN) metastatic patterns is not fully clear, especially following neoadjuvant chemotherapy (NAC). This study analyzed nodal metastatic patterns.
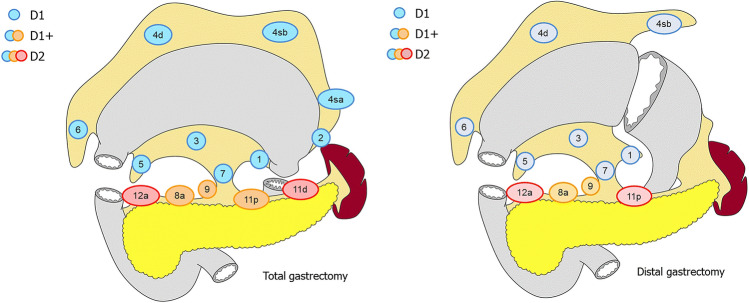
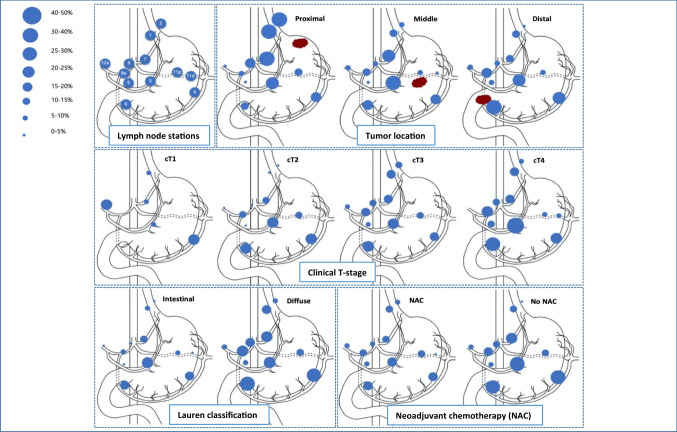
Methods: Individual LN stations were analyzed for all patients from the LOGICA-trial, a Dutch multicenter randomized trial comparing laparoscopic versus open D2-gastrectomy for gastric cancer. The pattern of metastases per LN station was related to tumor location, cT-stage, Lauren classification and NAC.
Results: Between 2015-2018, 212 patients underwent D2-gastrectomy, of whom 158 (75%) received NAC. LN metastases were present in 120 patients (57%). Proximal tumors metastasized predominantly to proximal LN stations (no. 1, 2, 7 and 9; p < 0.05), and distal tumors to distal LN stations (no. 5, 6 and 8; OR > 1, p > 0.05). However, distal tumors also metastasized to proximal LN stations, and vice versa. Despite NAC, each LN station (no. 1-9, 11 and 12a) showed metastases, regardless of tumor location, cT-stage, histological subtype and NAC treatment, including station 12a for cT1N0-tumors. LN metastases were present more frequently in diffuse versus intestinal tumors (66% versus 52%; p = 0,048), but not for cT3-4- versus cT1-2-stage (59% versus 51%; p = 0.259). However, the pattern of LN metastases was similar for these subgroups.
Conclusions: The extent of lymphadenectomy cannot be reduced after NAC for gastric cancer. Although the pattern of LN metastases is related to tumor location, all LN stations contained metastases regardless of tumor location, cT-stage (including cT1N0-tumors), histological subtype, or NAC treatment. Therefore, D2-lymphadenectomy should be routinely performed during gastrectomy in Western patients.
Keywords: Gastric cancer; Lymph node metastasis; Lymphadenectomy; Personalized medicine.
© 2022. The Author(s).
Conflict of interest statement
Richard van Hillegersberg: consulting or advisory role: Intuitive Surgical, Medtronic. Jelle Ruurda: consulting or advisory role: Intuitive Surgical. Lodewijk Brosens: advisory role: Bristol Myers Squibb. Misha Luyer: consulting or advisory role: Galvani, Medtronic. Research Funding: Dutch Cancer Foundation. Travel, Accommodations, and Expenses: Medtronic.
Figures

Similar articles
-
Clinicopathological Factors Predisposing to No. 12a Lymph Node Metastasis in Gastric Cancer: A Prospective Cohort Analysis.Cancer Rep (Hoboken). 2025 Jun;8(6):e70239. doi: 10.1002/cnr2.70239. Cancer Rep (Hoboken). 2025. PMID: 40498647 Free PMC article.
-
Clinical implications of the histologically and immunohistochemically detected solitary lymph node metastases in gastric cancer.Scand J Surg. 2011;100(3):174-80. doi: 10.1177/145749691110000307. Scand J Surg. 2011. PMID: 22108745
-
Assessment of Lymph Node Metastasis in Patients With Gastric Cancer to Identify Those Suitable for Middle Segmental Gastrectomy.JAMA Netw Open. 2021 Mar 1;4(3):e211840. doi: 10.1001/jamanetworkopen.2021.1840. JAMA Netw Open. 2021. PMID: 33729506 Free PMC article.
-
Prevalence of nodal metastases in the individual lymph node stations for different T-stages in gastric cancer: a systematic review.Updates Surg. 2023 Feb;75(2):281-290. doi: 10.1007/s13304-022-01347-w. Epub 2022 Aug 13. Updates Surg. 2023. PMID: 35962278 Free PMC article.
-
Neoadjuvant chemotherapy for gastric cancer. Is it a must or a fake?World J Gastroenterol. 2018 Jan 14;24(2):274-289. doi: 10.3748/wjg.v24.i2.274. World J Gastroenterol. 2018. PMID: 29375213 Free PMC article. Review.
Cited by
-
Assessment of the efficacy and safety of carbon nanoparticles-guided lymph node dissection in gastric cancer surgery: a systematic review and meta-analysis.Int J Clin Oncol. 2023 Jun;28(6):764-776. doi: 10.1007/s10147-023-02333-x. Epub 2023 Apr 26. Int J Clin Oncol. 2023. PMID: 37099219
-
Evaluating log odds of positive lymph nodes as a prognostic tool in differentiated gastric cancer: A retrospective study.World J Gastroenterol. 2025 Jun 7;31(21):107029. doi: 10.3748/wjg.v31.i21.107029. World J Gastroenterol. 2025. PMID: 40538517 Free PMC article.
-
The artificial intelligence revolution in gastric cancer management: clinical applications.Cancer Cell Int. 2025 Mar 21;25(1):111. doi: 10.1186/s12935-025-03756-4. Cancer Cell Int. 2025. PMID: 40119433 Free PMC article. Review.
-
Is No. 12a Lymph Node Dissection Compliance Necessary in Patients Who Undergo D2 Gastrectomy for Gastric Adenocarcinomas? A Population-Based Retrospective Propensity Score Matching Study.Cancers (Basel). 2023 Jan 25;15(3):749. doi: 10.3390/cancers15030749. Cancers (Basel). 2023. PMID: 36765707 Free PMC article.
-
[Evidence for the extent and oncological benefit of lymphadenectomy in gastric cancer].Chirurgie (Heidelb). 2025 Apr;96(4):281-287. doi: 10.1007/s00104-024-02198-4. Epub 2024 Dec 6. Chirurgie (Heidelb). 2025. PMID: 39643668 Review. German.
References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. - PubMed
-
- Hartgrink HH, van de Velde CJH, Putter H, Bonenkamp JJ, Klein Kranenbarg E, Songun I, et al. Extended lymph node dissection for gastric cancer: Who may benefit? Final results of the randomized Dutch Gastric Cancer Group Trial. J Clin Oncol. 2004;22(11):2069–2077. doi: 10.1200/JCO.2004.08.026. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
