

Racial Disparities in Outcomes After THA and TKA Are Substantially Mediated by Socioeconomic Disadvantage Both in Black and White Patients
- PMID: 36103368
- PMCID: PMC9831172
- DOI: 10.1097/CORR.0000000000002392
Racial Disparities in Outcomes After THA and TKA Are Substantially Mediated by Socioeconomic Disadvantage Both in Black and White Patients
Abstract
Background: Demographic factors have been implicated in THA and TKA outcome disparities. Specifically, patients' racial backgrounds have been reported to influence outcomes after surgery, including length of stay, discharge disposition, and inpatient readmissions. However, in the United States, health-impacting socioeconomic disadvantage is sometimes associated with racial differences in ways that can result in important confounding, thereby raising the question of whether race-associated post-THA/TKA adverse outcomes are an independent function of race or a byproduct of confounding from socioeconomic deprivation, which is potentially addressable. To explore this, we used the Area Deprivation Index (ADI) as a proxy for socioeconomic disadvantage, since it is a socioeconomic parameter that estimates the likely deprivation associated with a patient's home address.
Questions/purposes: The goal of this study was to investigate (1) whether race (in this study, Black versus White) was independently associated with adverse outcomes, including prolonged length of stay (LOS > 3 days), nonhome discharge, 90-day readmission, and emergency department (ED) visits while controlling for age, gender, BMI, smoking, Charlson comorbidity index (CCI), and insurance; and (2) whether socioeconomic disadvantage, measured by ADI, substantially mediated any association between race and any of the aforementioned measured outcomes.
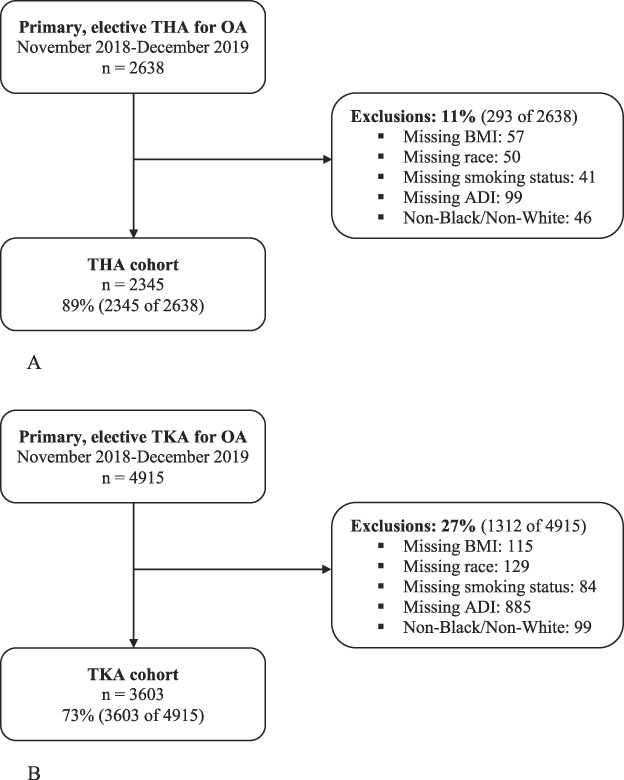
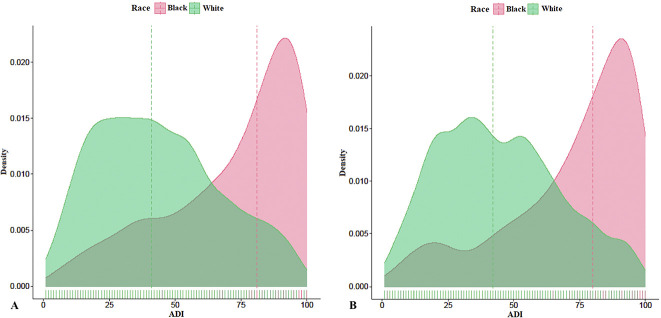
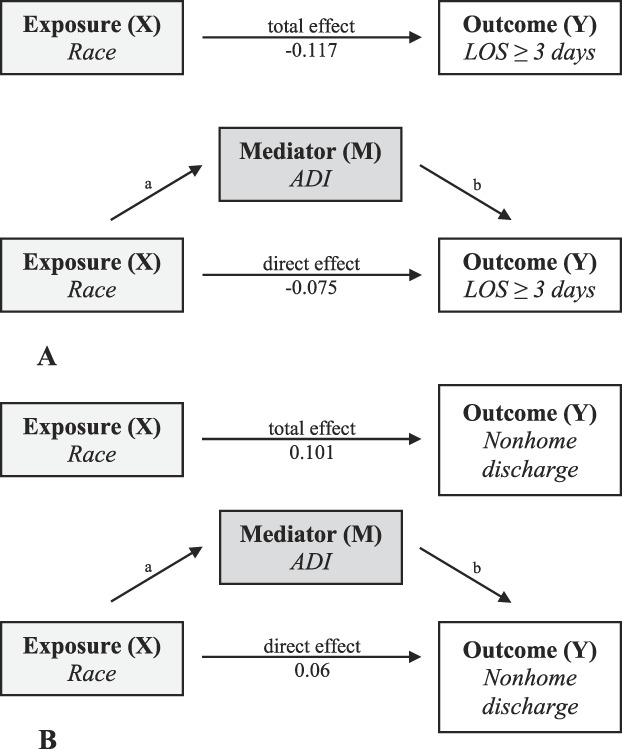
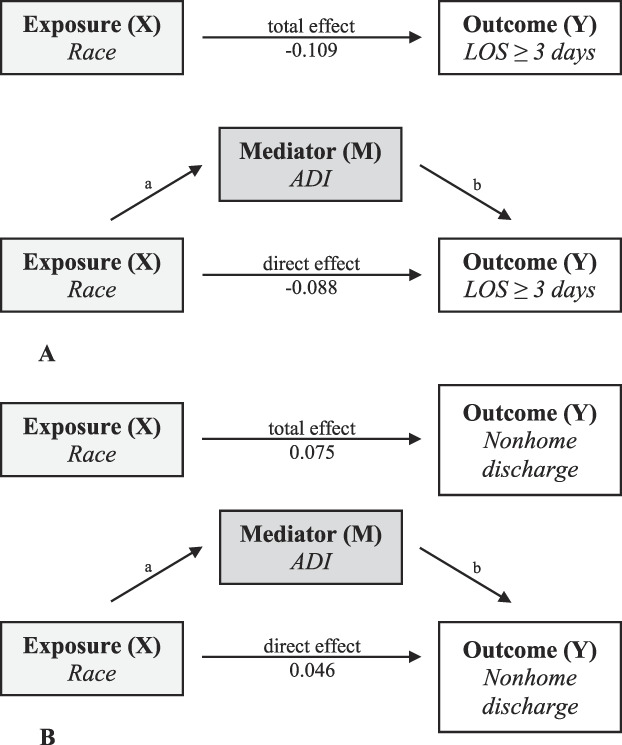
Methods: Between November 2018 and December 2019, 2638 underwent elective primary THA and 4915 patients underwent elective primary TKA for osteoarthritis at one of seven hospitals within a single academic center. Overall, 12% (742 of 5948) of patients were Black and 88% (5206 of 5948) were White. We included patients with complete demographic data, ADI data, and who were of Black or White race; with these criteria, 11% (293 of 2638) were excluded in the THA group, and 27% (1312 of 4915) of patients were excluded in the TKA group. In this retrospective, comparative study, patient follow-up was obtained using a longitudinally maintained database, leaving 89% (2345 of 2638) and 73% (3603 of 4915) for analysis in the THA and TKA groups, respectively. For both THA and TKA, Black patients had higher ADI scores, slightly higher BMIs, and were more likely to be current smokers at baseline. Furthermore, within the TKA cohort there was a higher proportion of Black women compared with White women. Multivariable regression analysis was utilized to assess associations between race and LOS of 3 or more days, nonhome discharge disposition, 90-day inpatient readmission, and 90-day ED admission, while adjusting for age, gender, BMI, smoking, CCI, and insurance. This was followed by a mediation analysis that explored whether the association between race (the independent variable) and measured outcomes (the dependent variables) could be partially or completely attributable to confounding from the ADI (the mediator, in this model). The mediation effect was measured as a percentage of the total effect of race on the outcomes of interest that was mediated by ADI.
Results: In the THA group, after adjusting for age, gender, BMI, smoking, CCI, and insurance, White patients had lower odds of experiencing an LOS of 3 days or more (OR 0.43 [95% confidence interval (CI) 0.31 to 0.59]; p < 0.001) and nonhome discharge (OR 0.39 [95% CI 0.27 to 0.56]; p < 0.001). In mediation analysis, ADI partially explained (or mediated) 37% of the association between race and LOS of 3 days or more (-0.043 [95% CI -0.063 to -0.026]; p < 0.001) and 40% of the association between race and nonhome discharge (0.041 [95% CI 0.024 to 0.059]; p < 0.001). However, a smaller direct association between race and both outcomes was observed (LOS 3 days or more: -0.075 [95% CI -0.13 to -0.024]; p = 0.004; nonhome discharge: 0.060 [95% CI 0.016 to 0.11]; p = 0.004). No association was observed between race and 90-day readmission or ED admission in the THA group. In the TKA group, after adjusting for age, gender, BMI, smoking, CCI, and insurance, White patients had lower odds of experiencing an LOS of 3 days or more (OR 0.41 [95% CI 0.32 to 0.54]; p < 0.001), nonhome discharge (OR 0.44 [95% CI 0.33 to 0.60]; p < 0.001), 90-day readmission (OR 0.54 [95% CI 0.39 to 0.77]; p < 0.001), and 90-day ED admission (OR 0.60 [95% CI 0.45 to 0.79]; p < 0.001). In mediation analysis, ADI mediated 19% of the association between race and LOS of 3 days or more (-0.021 [95% CI -0.035 to -0.007]; p = 0.004) and 38% of the association between race and nonhome discharge (0.029 [95% CI -0.016 to 0.040]; p < 0.001), but there was also a direct association between race and these outcomes (LOS 3 days or more: -0.088 [95% CI -0.13 to -0.049]; p < 0.001; nonhome discharge: 0.046 [95% CI 0.014 to 0.078]; p = 0.006). ADI did not mediate the associations observed between race and 90-day readmission and ED admission in the TKA group.
Conclusion: Our findings suggest that socioeconomic disadvantage may be implicated in a substantial proportion of the previously assumed race-driven disparity in healthcare utilization parameters after primary total joint arthroplasty. Orthopaedic surgeons should attempt to identify potentially modifiable socioeconomic disadvantage indicators. This serves as a call to action for the orthopaedic community to consider specific interventions to support patients from vulnerable areas or whose incomes are lower, such as supporting applications for nonemergent medical transportation or referring patients to local care coordination agencies. Future studies should seek to identify which specific resources or approaches improve outcomes after TJA in patients with socioeconomic disadvantage.
Level of evidence: Level III, therapeutic study.
Copyright © 2022 by the Association of Bone and Joint Surgeons.
Conflict of interest statement
The authors certify that there are no funding or commercial associations (consultancies, stock ownership, equity interest, patent/licensing arrangements, etc.) that might pose a conflict of interest in connection with the submitted article related to the author or any immediate family members. All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research ® editors and board members are on file with the publication and can be viewed on request.
Figures
Comment in
-
CORR Insights®: Racial Disparities in Outcomes After THA and TKA Are Substantially Mediated by Socioeconomic Disadvantage Both in Black and White Patients.Clin Orthop Relat Res. 2023 Feb 1;481(2):265-267. doi: 10.1097/CORR.0000000000002452. Epub 2022 Oct 11. Clin Orthop Relat Res. 2023. PMID: 36219039 Free PMC article. No abstract available.
Similar articles
-
NarxCare Scores Greater Than 300 Are Associated with Adverse Outcomes After Primary THA.Clin Orthop Relat Res. 2021 Sep 1;479(9):1957-1967. doi: 10.1097/CORR.0000000000001745. Clin Orthop Relat Res. 2021. PMID: 33835083 Free PMC article.
-
Neighborhood Socioeconomic Disadvantage is Associated With Increased Health Care Utilization After Septic and Aseptic Revision Total Hip Arthroplasty.J Arthroplasty. 2025 Mar;40(3):550-558.e2. doi: 10.1016/j.arth.2024.09.014. Epub 2024 Sep 16. J Arthroplasty. 2025. PMID: 39293696
-
Preoperative Colonization With Staphylococcus Aureus in THA Is Associated With Increased Length of Stay.Clin Orthop Relat Res. 2022 Aug 1;480(8):1504-1514. doi: 10.1097/CORR.0000000000002136. Epub 2022 Feb 7. Clin Orthop Relat Res. 2022. PMID: 35130192 Free PMC article.
-
Racial and Ethnic Disparities in Total Joint Arthroplasty Care: A Contemporary Systematic Review and Meta-Analysis.J Arthroplasty. 2023 Jan;38(1):171-187.e18. doi: 10.1016/j.arth.2022.08.006. Epub 2022 Aug 17. J Arthroplasty. 2023. PMID: 35985539
-
Factors associated with hospital stay length, discharge destination, and 30-day readmission rate after primary hip or knee arthroplasty: Retrospective Cohort Study.Orthop Traumatol Surg Res. 2019 Sep;105(5):949-955. doi: 10.1016/j.otsr.2019.04.012. Epub 2019 Jun 15. Orthop Traumatol Surg Res. 2019. PMID: 31208932 Review.
Cited by
-
Healthcare disparities: patients' perspectives on barriers to joint replacement.BMC Musculoskelet Disord. 2023 Dec 18;24(1):976. doi: 10.1186/s12891-023-07096-0. BMC Musculoskelet Disord. 2023. PMID: 38110904 Free PMC article.
-
The effect of Charlson Comorbidity Index, race, and surgical complications on postoperative knee outcomes after total knee arthroplasty.Arch Orthop Trauma Surg. 2025 Apr 19;145(1):255. doi: 10.1007/s00402-025-05867-z. Arch Orthop Trauma Surg. 2025. PMID: 40252121 Free PMC article.
-
Disparities Exist in the Experience of Financial Burden Among Orthopedic Trauma Patients: A Systematic Review.Curr Rev Musculoskelet Med. 2024 May;17(5):129-135. doi: 10.1007/s12178-024-09890-2. Epub 2024 Mar 16. Curr Rev Musculoskelet Med. 2024. PMID: 38491251 Free PMC article. Review.
-
The Investigation of Preoperative Factors Associated With Postoperative Outcomes Following Total Knee Arthroplasty for Osteoarthritis: A Scoping Review.Cureus. 2024 Jul 20;16(7):e64989. doi: 10.7759/cureus.64989. eCollection 2024 Jul. Cureus. 2024. PMID: 39161506 Free PMC article.
-
Healthcare disparities in adult and pediatric spinal deformity: a state of the art review.Spine Deform. 2025 Mar;13(2):373-381. doi: 10.1007/s43390-024-01012-9. Epub 2024 Nov 27. Spine Deform. 2025. PMID: 39602061 Review.
References
-
- Agabiti N, Picciotto S, Cesaroni G, et al. The influence of socioeconomic status on utilization and outcomes of elective total hip replacement: a multicity population-based longitudinal study. Int J Qual Health Care. 2007;19:37-44. - PubMed
-
- Alvarez PM, McKeon JF, Spitzer AI, et al. Race, utilization, and outcomes in total hip and knee arthroplasty: a systematic review on health-care disparities. JBJS Rev. 2022;10:e21.00161. - PubMed
-
- Amen TB, Varady NH, Rajaee S, Chen AF. Persistent racial disparities in utilization rates and perioperative metrics in total joint arthroplasty in the U.S. J Bone Joint Surg Am. 2020;102:811-820. - PubMed
-
- Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40:373-383. - PubMed
-
- Courtney PM, Huddleston JI, Iorio R, Markel DC. Socioeconomic risk adjustment models for reimbursement are necessary in primary total joint arthroplasty. J Arthroplasty. 2017;32:1-5. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
