

Disentangling the cognitive, physical, and mental health sequelae of COVID-19
- PMID: 36103880
- PMCID: PMC9448696
- DOI: 10.1016/j.xcrm.2022.100750
Disentangling the cognitive, physical, and mental health sequelae of COVID-19
Abstract
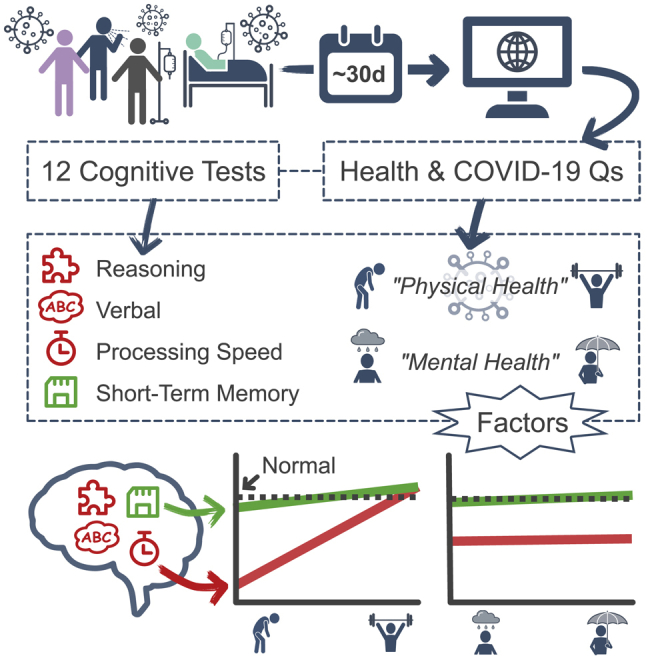
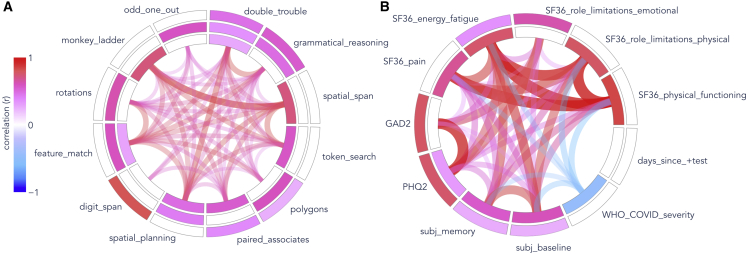
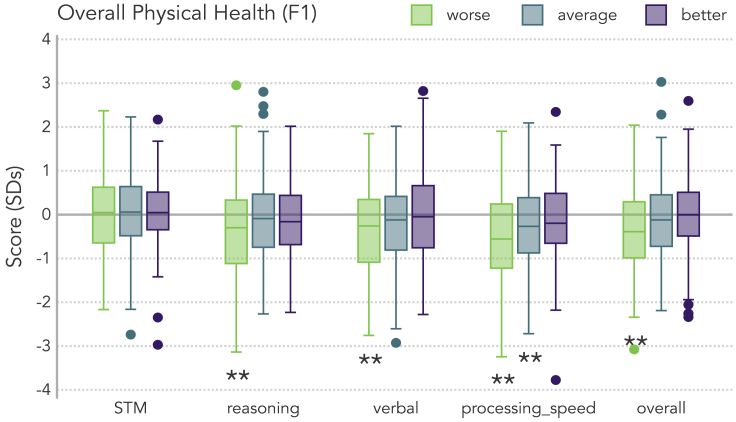
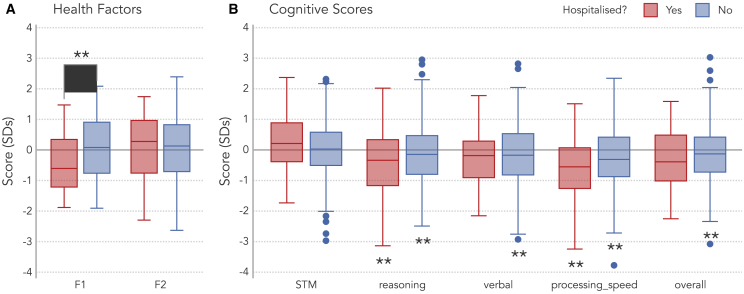
As COVID-19 cases exceed hundreds of millions globally, many survivors face cognitive challenges and prolonged symptoms. However, important questions about the cognitive effects of COVID-19 remain unresolved. In this cross-sectional online study, 478 adult volunteers who self-reported a positive test for COVID-19 (mean = 30 days since most recent test) perform significantly worse than pre-pandemic norms on cognitive measures of processing speed, reasoning, verbal, and overall performance, but not short-term memory, suggesting domain-specific deficits. Cognitive differences are even observed in participants who did not require hospitalization. Factor analysis of health- and COVID-related questionnaires reveals two clusters of symptoms-one that varies mostly with physical symptoms and illness severity, and one with mental health. Cognitive performance is positively correlated with the global measure encompassing physical symptoms, but not the one that broadly describes mental health, suggesting that the subjective experience of "long COVID" relates to physical symptoms and cognitive deficits, especially executive dysfunction.
Keywords: COVID-19; cognition; cross-sectional online study; long COVID; mental health; physical health.
Copyright © 2022 The Author(s). Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of interests The cognitive tests used in this study are marketed by Cambridge Brain Sciences (CBS), of which A.M.O. is the chief scientific officer. Under the terms of the existing licensing agreement, A.M.O. and his collaborators are free to use the platform at no cost for their scientific studies, and that such research projects neither contribute to, nor are influenced by, the activities of the company. C.J.W. provides consulting services to CBS. Consequently, there is no overlap between the present study and the activities of CBS, nor was there any cost to the authors, funding bodies, or participants who were involved in the study. R.H.S. is founder and owner of FollowMD, Inc., a vascular risk-reduction clinic. The authors declare no other competing interests.
Figures
References
-
- Wild C.J., Norton L., Swartz R.H., Owen A.M. Cognitive testing and questionnaire data from survivors of COVID-19. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
