

Proactive esophageal cooling protects against thermal insults during high-power short-duration radiofrequency cardiac ablation
- PMID: 36104029
- PMCID: PMC9771690
- DOI: 10.1080/02656736.2022.2121860
Proactive esophageal cooling protects against thermal insults during high-power short-duration radiofrequency cardiac ablation
Abstract
Background: Proactive cooling with a novel cooling device has been shown to reduce endoscopically identified thermal injury during radiofrequency (RF) ablation for the treatment of atrial fibrillation using medium power settings. We aimed to evaluate the effects of proactive cooling during high-power short-duration (HPSD) ablation.
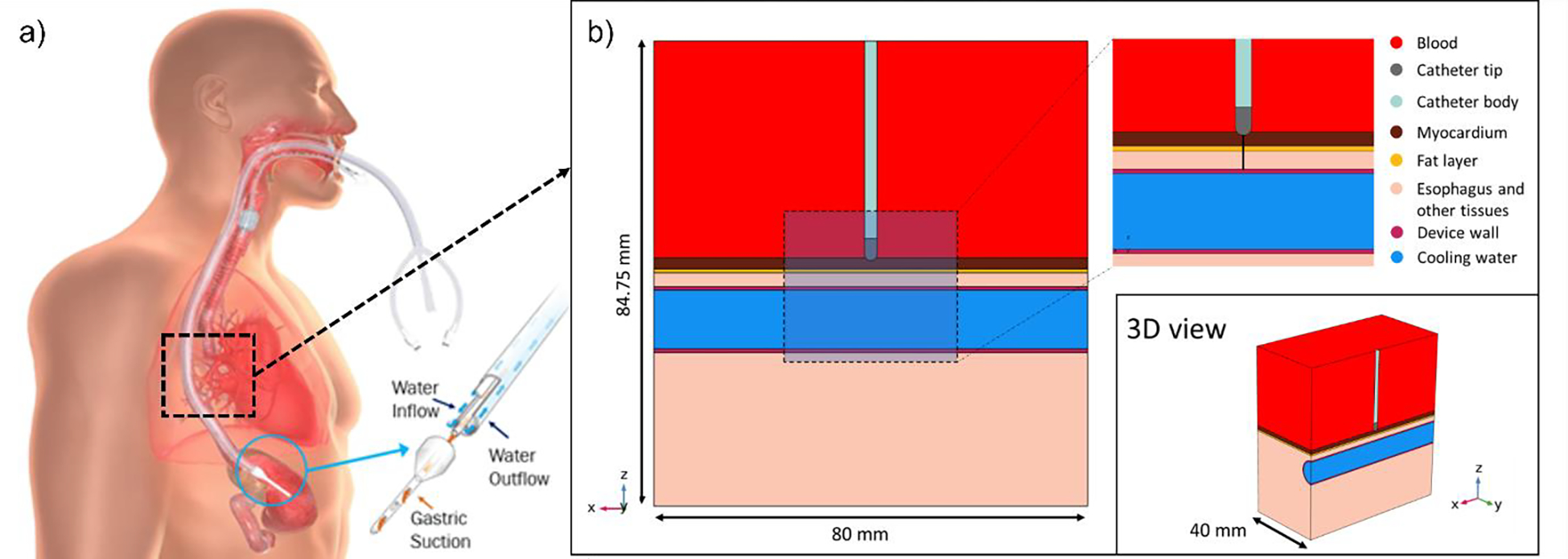
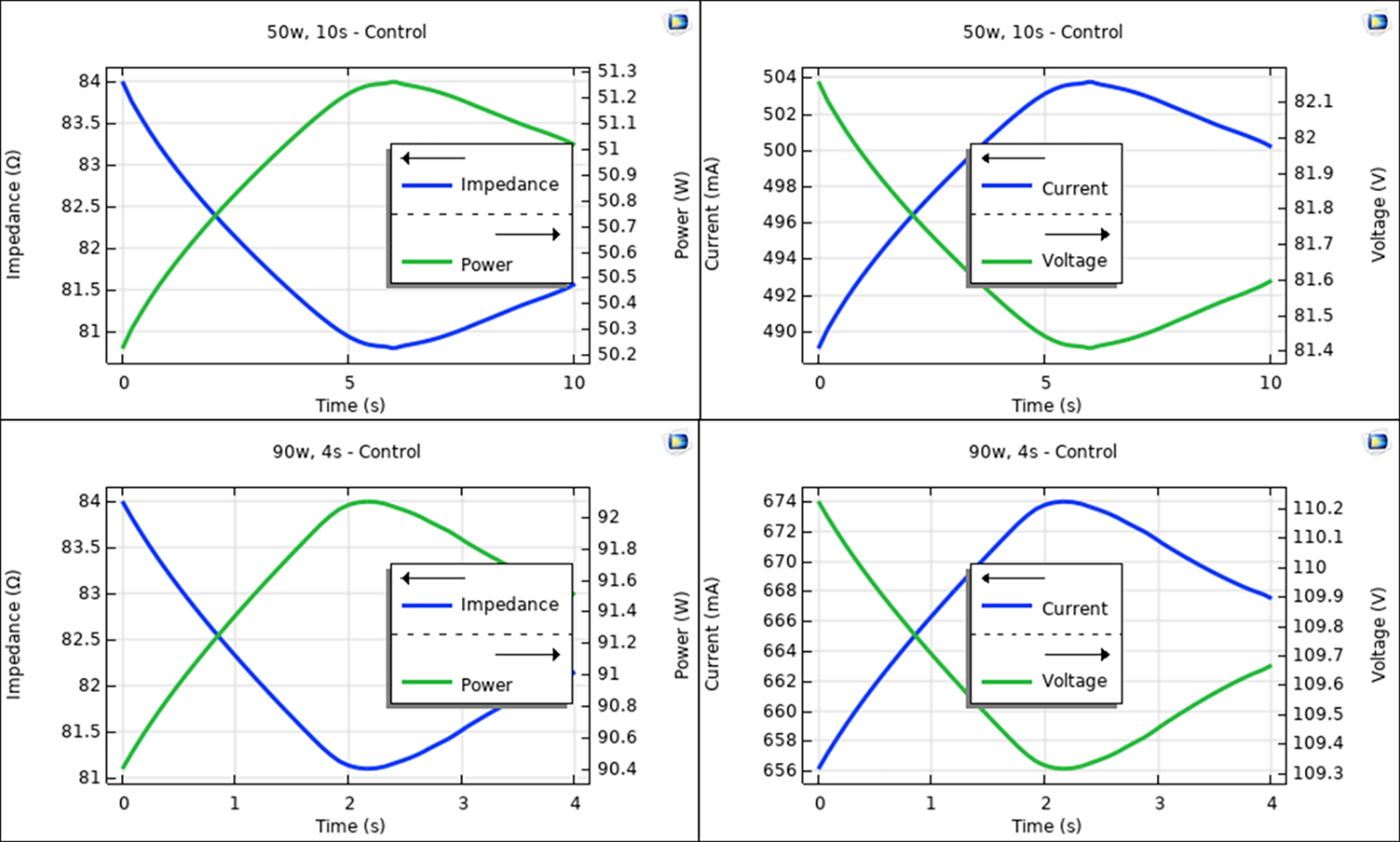
Methods: A computer model accounting for the left atrium (1.5 mm thickness) and esophagus including the active cooling device was created. We used the Arrhenius equation to estimate the esophageal thermal damage during 50 W/ 10 s and 90 W/ 4 s RF ablations.
Results: With proactive esophageal cooling in place, temperatures in the esophageal tissue were significantly reduced from control conditions without cooling, and the resulting percentage of damage to the esophageal wall was reduced around 50%, restricting damage to the epi-esophageal region and consequently sparing the remainder of the esophageal tissue, including the mucosal surface. Lesions in the atrial wall remained transmural despite cooling, and maximum width barely changed (<0.8 mm).
Conclusions: Proactive esophageal cooling significantly reduces temperatures and the resulting fraction of damage in the esophagus during HPSD ablation. These findings offer a mechanistic rationale explaining the high degree of safety encountered to date using proactive esophageal cooling, and further underscore the fact that temperature monitoring is inadequate to avoid thermal damage to the esophagus.
Keywords: Atrial fibrillation; atrioesophageal fistula; esophageal cooling; mathematical modeling; radiofrequency ablation.
Conflict of interest statement
Figures





References
-
- Della Rocca DG, Magnocavallo M, Natale VN, Gianni C, Mohanty S, Trivedi C, Lavalle C, Forleo GB, Tarantino N, Romero J, Zhang X, Bassiouny M, Al-Ahmad A, Burkhardt DJ, Gallinghouse JG, Sanchez JE, Horton RP, Di Biase L, Natale A. Clinical presentation, diagnosis, and treatment of atrioesophageal fistula resulting from atrial fibrillation ablation. J Cardiovasc Electrophysiol. 2021. Sep;32(9):2441–2450. doi: 10.1111/jce.15168. - DOI - PubMed
-
- Andrade JG, Champagne J, Dubuc M, Deyell MW, Verma A, Macle L, Leong-Sit P, Novak P, Badra-Verdu M, Sapp J, Mangat I, Khoo C, Steinberg C, Bennett MT, Tang ASL, Khairy P; CIRCA-DOSE Study Investigators. Cryoballoon or Radiofrequency Ablation for Atrial Fibrillation Assessed by Continuous Monitoring: A Randomized Clinical Trial. Circulation. 2019. Nov 26;140(22):1779–1788. doi: 10.1161/CIRCULATIONAHA.119.042622. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical