

Outcome of giant pituitary tumors requiring surgery
- PMID: 36105410
- PMCID: PMC9465329
- DOI: 10.3389/fendo.2022.975560
Outcome of giant pituitary tumors requiring surgery
Abstract
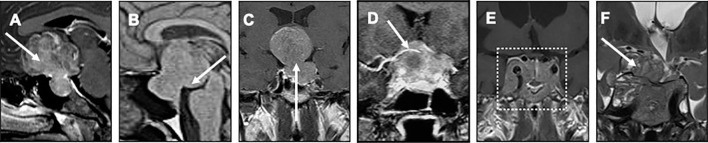
Objective: The management of giant pituitary tumors is complex, with few publications and recommendations. Consequently, patient's care mainly relies on clinical experience. We report here a first large series of patients with giant pituitary tumors managed by a multidisciplinary expert team, focusing on treatments and outcome.
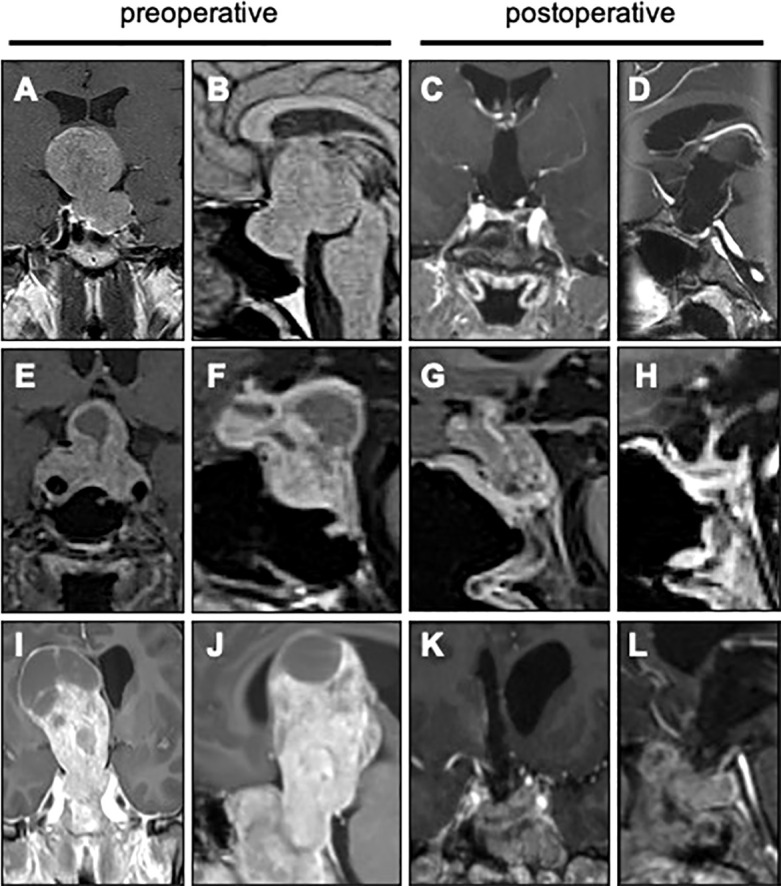
Methods: A retrospective cohort study was conducted. Giant pituitary tumors were defined by a main diameter > 40mm. Macroprolactinomas sensitive to dopamine agonists were excluded. All patients were operated by a single neurosurgical team. After surgery, multimodal management was proposed, including hormone replacement, radiotherapy and anti-tumor medical therapies. Outcome was modeled using Kaplan-Meyer representation. A logistic regression model was built to identify the risk factors associated with surgical complications.
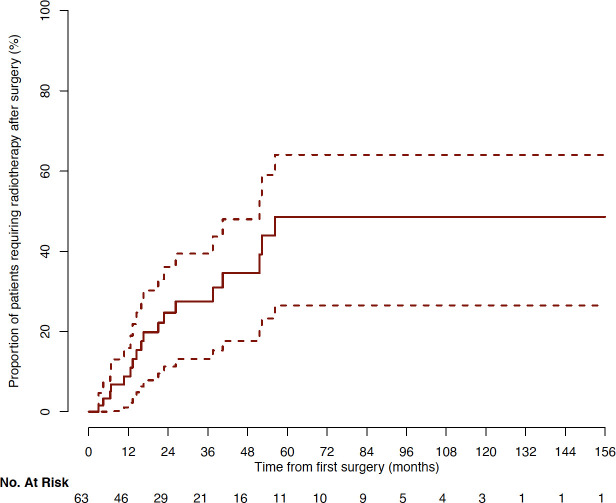
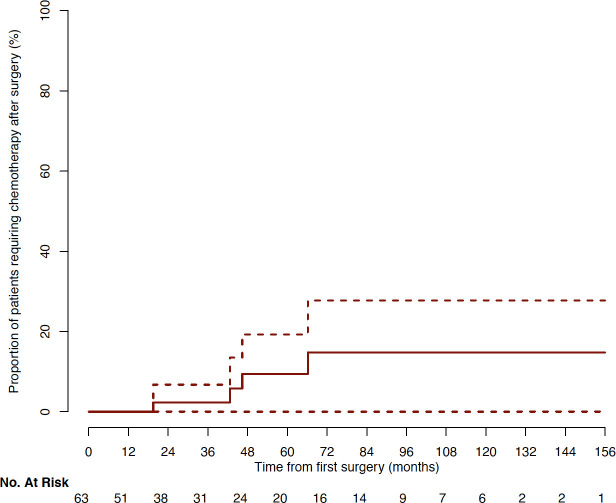
Results: 63 consecutive patients presented a giant adenoma, most often with visual defects. Patients were operated once, twice or three times in 59%, 40% and 1% of cases respectively, mainly through endoscopic endonasal approach. Giant adenomas included gonadotroph, corticotroph, somatotroph, lactotroph and mixed GH-PRL subtypes in 67%, 14%, 11%, 6% and 2% of patients respectively. Vision improved in 89% of patients with prior visual defects. Severe surgical complications occurred in 11% of patients, mainly for tumors > 50 mm requiring microscopic transcranial approach. Additional radiotherapy was needed for 29% of patients, 3 to 56 months after first surgery. For 6% of patients, Temozolomide treatment was required, 19 to 66 months after first surgery.
Conclusions: Giant pituitary tumors require multimodal management, with a central role of surgery. Most often, tumor control can be achieved by expert multidisciplinary teams.
Keywords: adenoma; aggressiveness; complication; giant pituitary tumor; radiotherapy; surgery.
Copyright © 2022 Gaillard, Adeniran, Villa, Jouinot, Raffin-Sanson, Feuvret, Verrelle, Bonnet, Dohan, Bertherat, Assié and Baussart.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical