

The impact of diagnosed fetal anomaly, diagnostic severity and prognostic ambiguity on parental depression and traumatic stress: a prospective longitudinal cohort study
- PMID: 36106375
- PMCID: PMC9812208
- DOI: 10.1111/aogs.14453
The impact of diagnosed fetal anomaly, diagnostic severity and prognostic ambiguity on parental depression and traumatic stress: a prospective longitudinal cohort study
Abstract
Introduction: The detection of a fetal anomaly during routine obstetric ultrasound is a potentially traumatic experience. The aim of this study is to examine longitudinally the impact of diagnosis of fetal anomaly on symptoms of depression and traumatic stress among mothers and fathers, and to examine how variations in psychological adjustment relate to diagnostic severity and prognostic ambiguity.
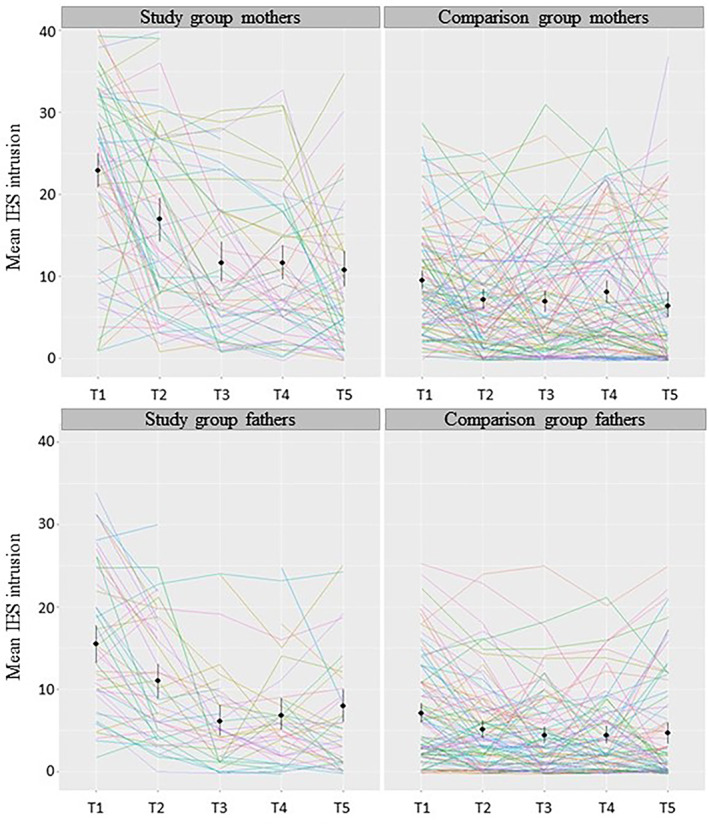
Material and methods: In this prospective observational study conducted at a tertiary perinatal referral center, 81 mothers and 69 fathers with ultrasound findings of fetal anomaly completed the Edinburgh Postnatal Depression Scale (EPDS) and Impact of Events Scale (IES) at four time points in pregnancy (T1-T4) and 6 weeks after birth (T5). We compared this with depression and traumatic stress in a sample of non-affected parents (n = 110 mothers, 98 fathers).
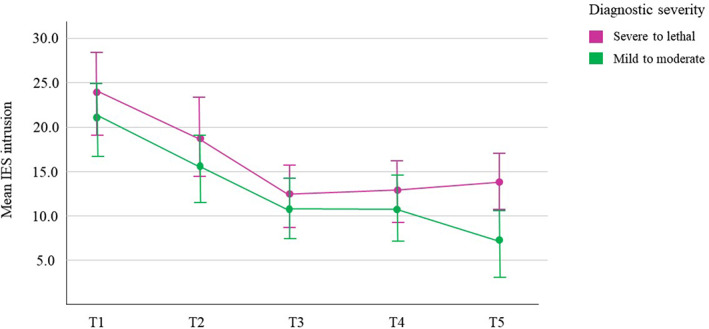
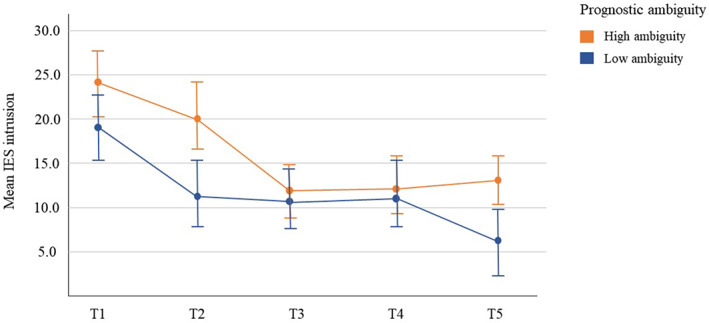
Results: Linear mixed effects models indicated that parents who received a diagnosis of fetal anomaly experienced higher levels of depression and traumatic stress over time, compared with non-affected parents. Depression: mean difference mothers = 4.46 ± 0.47, fathers = 2.80 ± 0.42. Traumatic stress: mean difference mothers = 20.04 ± 2.13, fathers = 12.66 ± 1.74. Parents with a more severe diagnosis experienced elevated symptoms compared with parents with a less severe diagnosis. Among mothers, prognostic ambiguity and changes in the anticipated diagnosis after birth were also associated with increased distress, regardless of whether the change was for the better or worse.
Conclusions: Diagnosis of fetal anomaly increases risk of depression and traumatic stress in expectant mothers and fathers, both acutely and over time.
Keywords: congenital malformation; depression; postpartum; pregnancy; prenatal diagnosis; psychological distress; traumatic stress.
© 2022 The Authors. Acta Obstetricia et Gynecologica Scandinavica published by John Wiley & Sons Ltd on behalf of Nordic Federation of Societies of Obstetrics and Gynecology (NFOG).
Conflict of interest statement
The authors have stated explicitly that there are no conflicts of interest in connection with this article.
Figures
Similar articles
-
Long-Term Impact of Diagnosed Fetal Anomaly on Parental Traumatic Stress, Resilience, and Relationship Satisfaction.J Pediatr Psychol. 2023 Feb 21;48(2):181-192. doi: 10.1093/jpepsy/jsac085. J Pediatr Psychol. 2023. PMID: 36399086 Free PMC article.
-
Paternal psychological response after ultrasonographic detection of structural fetal anomalies with a comparison to maternal response: a cohort study.BMC Pregnancy Childbirth. 2013 Jul 12;13:147. doi: 10.1186/1471-2393-13-147. BMC Pregnancy Childbirth. 2013. PMID: 23845090 Free PMC article.
-
Antenatal depressive symptoms and subjective birth experience in association with postpartum depressive symptoms and acute stress reaction in mothers and fathers: A longitudinal path analysis.Eur J Obstet Gynecol Reprod Biol. 2017 Aug;215:68-74. doi: 10.1016/j.ejogrb.2017.05.021. Epub 2017 May 30. Eur J Obstet Gynecol Reprod Biol. 2017. PMID: 28601730
-
Perinatal loss and parental distress after the birth of a healthy infant.Adv Neonatal Care. 2007 Aug;7(4):200-6. doi: 10.1097/01.ANC.0000286337.90799.7d. Adv Neonatal Care. 2007. PMID: 17700194
-
New parents' experiences of postpartum depression: a systematic review of qualitative evidence.JBI Database System Rev Implement Rep. 2019 Sep;17(9):1731-1769. doi: 10.11124/JBISRIR-2017-003909. JBI Database System Rev Implement Rep. 2019. PMID: 31021977
Cited by
-
Prenatal Psychosocial Distress Screening for Individuals Experiencing Pregnancies Complicated by Fetal Anomalies.J Pers Med. 2025 Jul 18;15(7):322. doi: 10.3390/jpm15070322. J Pers Med. 2025. PMID: 40710439 Free PMC article.
-
Prenatal Diagnosis of Acrania in One Twin of a Dichorionic Diamniotic Pregnancy: A Case Report on Management and Perinatal Outcome.Reports (MDPI). 2025 May 22;8(2):75. doi: 10.3390/reports8020075. Reports (MDPI). 2025. PMID: 40710866 Free PMC article.
-
Communicating neurological prognosis in the prenatal period: a narrative review and practice guidelines.Pediatr Res. 2025 Jan 14. doi: 10.1038/s41390-025-03805-8. Online ahead of print. Pediatr Res. 2025. PMID: 39809859 Review.
-
Family dynamics after diagnosis and surgical treatment of myelomeningocele: using telemedicine as a complementary tool.Childs Nerv Syst. 2025 Aug 11;41(1):259. doi: 10.1007/s00381-025-06920-3. Childs Nerv Syst. 2025. PMID: 40789830 Review.
-
Harnessing the Power of Artificial Intelligence in Cleft Lip and Palate: An In-Depth Analysis from Diagnosis to Treatment, a Comprehensive Review.Children (Basel). 2024 Jan 23;11(2):140. doi: 10.3390/children11020140. Children (Basel). 2024. PMID: 38397252 Free PMC article. Review.
References
-
- Dolk H, Loane M, Garne E. The prevalence of congenital anomalies in Europe. Adv Exp Med Biol. 2010;686:349‐364. - PubMed
-
- Aite L, Zaccara A, Mirante N, et al. Antenatal diagnosis of congenital anomaly: a really traumatic experience? J Perinatol. 2011;31:760‐763. - PubMed
-
- Davies V, Gledhill J, McFadyen A, Whitlow B, Economides D. Psychological outcome in women undergoing termination of pregnancy for ultrasound‐detected fetal anomaly in the first and second trimesters: a pilot study. Ultrasound Obstet Gynecol. 2005;25:389‐392. - PubMed
-
- Kersting A, Kroker K, Steinhard J, et al. Psychological impact on women after second and third trimester termination of pregnancy due to fetal anomalies versus women after preterm birth—a 14‐month follow up study. Arch Womens Ment Health. 2009;12:193‐201. - PubMed
-
- Korenromp MJ, Page‐Christiaens GC, van den Bout J, Mulder EJ, Visser GH. Adjustment to termination of pregnancy for fetal anomaly: a longitudinal study in women at 4, 8, and 16 months. Am J Obstet Gynecol. 2009;201:160.e1‐e7. - PubMed
