

Gaps in the screening process for women diagnosed with cervical cancer in four diverse US health care settings
- PMID: 36106421
- PMCID: PMC9939213
- DOI: 10.1002/cam4.5226
Gaps in the screening process for women diagnosed with cervical cancer in four diverse US health care settings
Abstract
Background: Potential care gaps in the cervical cancer screening process among women diagnosed with cervical cancer in an era with increased human papillomavirus (HPV) testing have not been extensively evaluated.
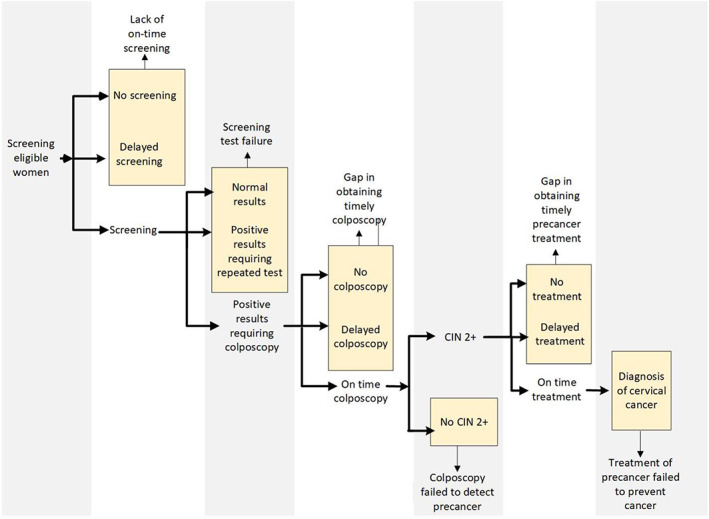
Methods: Women diagnosed with cervical cancer between ages 21 and 65 at four study sites between 2010 and 2014 were included. Screening histories were ascertained from 0.5 to 4 years prior to cervical cancer diagnosis. We identified potential care gaps in the screening history for each woman and classified them into one of three mutually exclusive types: lack of a screening test, screening test failure, and diagnostic/treatment care gap. Distributions of care gaps were tabulated by stage, histology, and study site. Multivariable nominal logistic regression was used to examine the associations between demographic and cancer characteristics and type of care gap.
Results: Of 499 women evaluated, 46% lacked a screening test in the time window examined, 31% experienced a screening test failure, and 22% experienced a diagnostic/treatment care gap. More than half of the women with advanced cancer and squamous cell carcinoma lacked a screening test compared to 31% and 24% of women with localized cancer and adenocarcinoma, respectively. Women aged 21-29 at diagnosis were more likely to experience screening test failure and diagnostic/treatment care gap, while those aged 50-65 were more likely to lack a screening test, compared to women aged 30-39.
Conclusions: Our findings demonstrate a continuing need to develop interventions targeting unscreened and under-screened women and improve detection and diagnosis of adenocarcinoma in women undergoing cervical cancer screening and diagnostic follow-up.
Keywords: cancer screening; cervical cancer; cervical cancer prevention; cervical cancer screening; health service research.
© 2022 The Authors. Cancer Medicine published by John Wiley & Sons Ltd.
Conflict of interest statement
In 2021, Dr. Chun Chao was the Principal Investigator of a contract from Merck & Co., Inc. awarded to the Kaiser Permanente Southern California on ovarian cancer management.
From 2019 to 2020, Dr. Jessica Chubak was the Principal Investigator of a contract from Amgen, Inc. awarded to the Kaiser Foundation Health Plan of Washington to evaluate the accuracy of using electronic health record data to identify individuals with reduced ejection fraction heart failure. Dr. Cossette M. Wheeler has received funds from grants cooperative agreements related to cervical cancer screening and triage through her institution, the University of New Mexico. Cossette M. Wheeler reports receiving reagents and equipment from Roche Molecular Systems, Roche/Ventana Medical Systems, Hologic and Genera Biosystem through their institution and outside of the submitted work, research support from Becton Dickinson (BD) and Hologic through her institution and outside of the submitted work, personal fees from BD also outside of the submitted work, personal fees from BD also outside of this work. Dr. Sarah Feldman authored chapters for Up‐to‐date and received honorarium for this activity.
Figures

References
-
- Practice bulletin no. 168: cervical cancer screening and prevention. Obstet Gynecol. 2016;128(4):e111‐e130. - PubMed
-
- Group USCSW. U.S . Cancer Statistics Data Visualizations Tool, based on November 2017 submission data (1999–2015). 2018; https://gis.cdc.gov/Cancer/USCS/DataViz.html. Accessed August 2018.
-
- Leyden WA, Manos MM, Geiger AM, et al. Cervical cancer in women with comprehensive health care access: attributable factors in the screening process. J Natl Cancer Inst. 2005;97(9):675‐683. - PubMed
-
- Priebe AM. 2012 cervical cancer screening guidelines and the future role of HPV testing. Clin Obstet Gynecol. 2013;56(1):44‐50. - PubMed
