

Acceptance of Different Self-sampling Methods for Semiweekly SARS-CoV-2 Testing in Asymptomatic Children and Childcare Workers at German Day Care Centers: A Nonrandomized Controlled Trial
- PMID: 36107424
- PMCID: PMC9478779
- DOI: 10.1001/jamanetworkopen.2022.31798
Acceptance of Different Self-sampling Methods for Semiweekly SARS-CoV-2 Testing in Asymptomatic Children and Childcare Workers at German Day Care Centers: A Nonrandomized Controlled Trial
Erratum in
-
Error in Figure 3.JAMA Netw Open. 2022 Oct 3;5(10):e2240161. doi: 10.1001/jamanetworkopen.2022.40161. JAMA Netw Open. 2022. PMID: 36223122 Free PMC article. No abstract available.
Abstract
Importance: Closure of day care centers (DCCs) to contain the COVID-19 pandemic has been associated with negative effects on children's health and well-being.
Objective: To investigate the acceptance of self-sampling methods for continuous SARS-CoV-2 surveillance among asymptomatic children and childcare workers (CCWs) in DCCs.
Design, setting, and participants: This nonrandomized pilot study included children and CCWs at 9 DCCs in Wuerzburg, Germany, from May to July 2021.
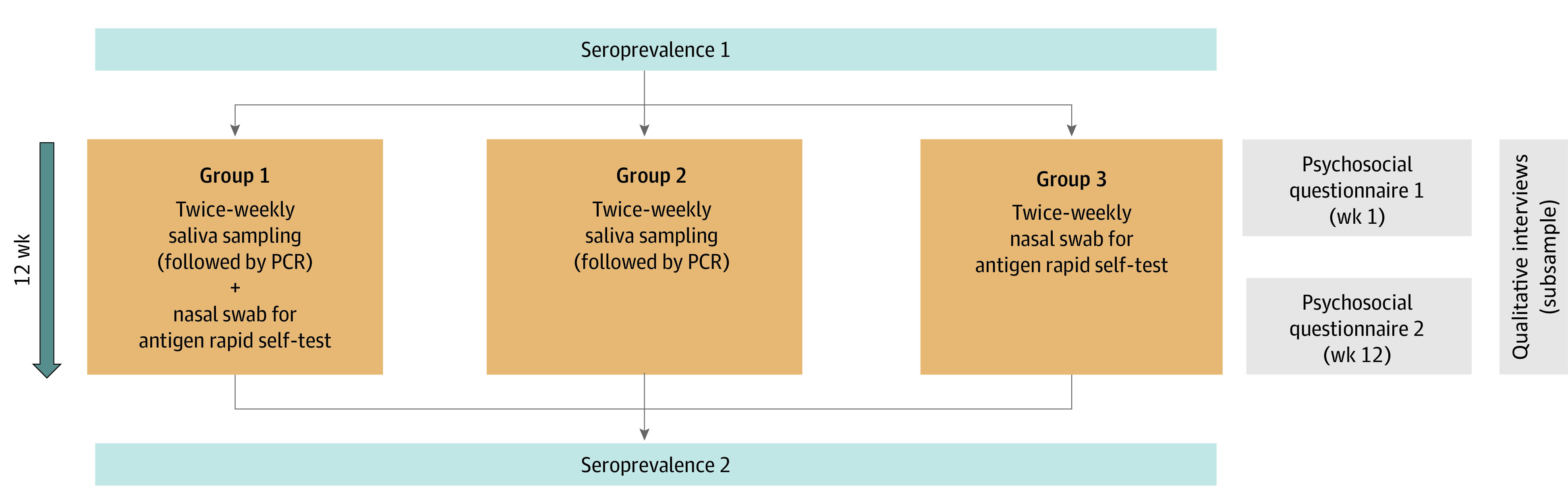
Interventions: Twice weekly testing for SARS-CoV-2 was conducted by self-sampled mouth-rinsing fluid (saliva sampling [SAL], with subsequent pooled polymerase chain reaction test) plus nasal rapid antigen self-test (RAgT) (group 1), SAL only (group 2), or RAgT only (group 3) in children and CCWs.
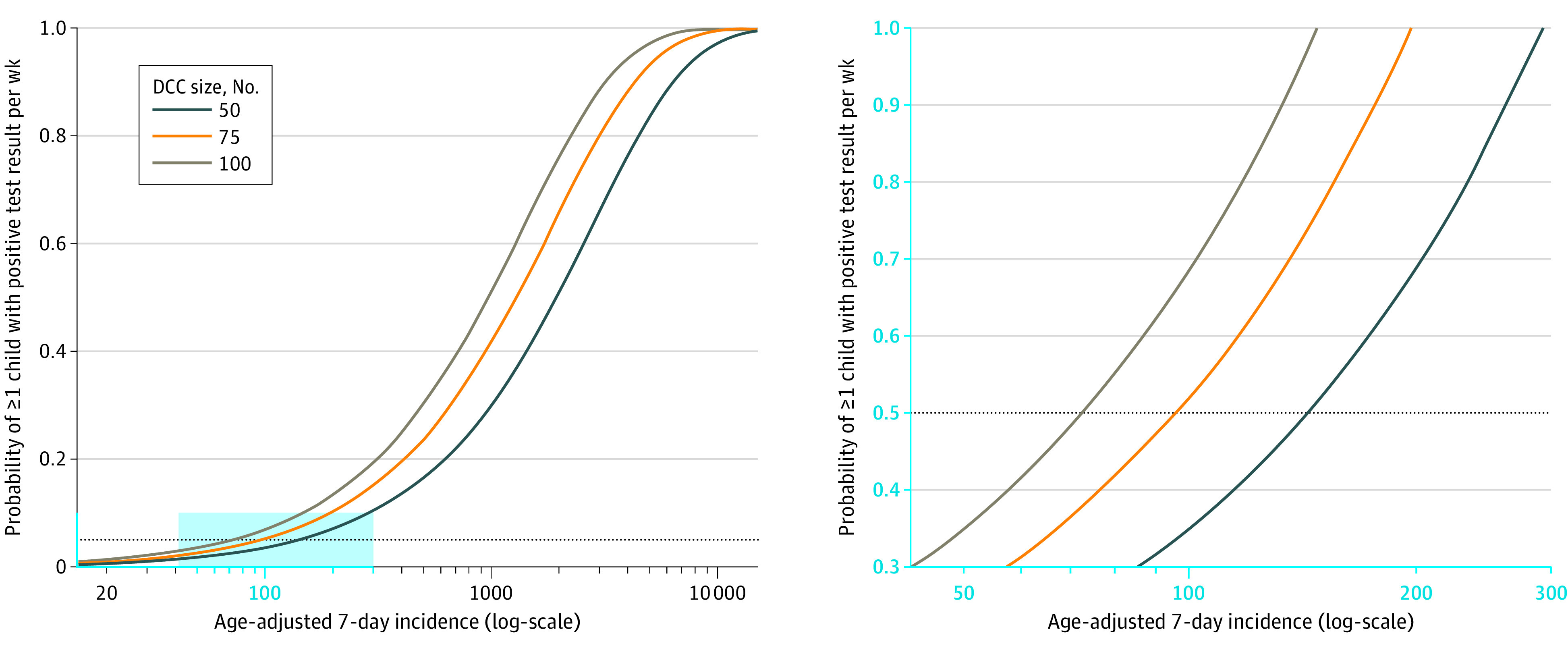
Main outcomes and measures: Main outcomes were rates for initial acceptance and successful (≥60% of scheduled samples) long-term participation. The probability of SARS-CoV-2 introduction into DCCs was modeled as a function of age-adjusted background incidence and DCC size.
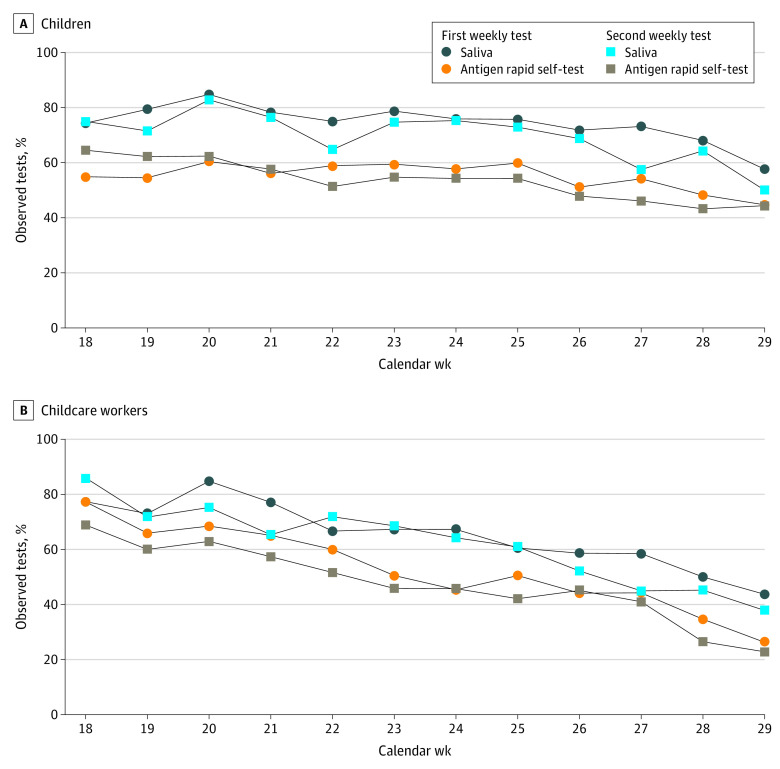
Results: Of 836 eligible children, 452 (54.1%; 95% CI, 50.7%-57.4%) participated (median [IQR] age: 4 [3-5] years; 213 [47.1%] girls), including 215 (47.6%) in group 1, 172 (38.1%) in group 2, and 65 (14.4%) in group 3. Of 190 CCWs, 139 (73.2%; 95% CI, 66.4%-79.0%) participated (median [IQR] age: 30 [25-46] years; 128 [92.1%] women), including 96 (69.1%) in group 1, 29 (20.9%) in group 2, and 14 (10.1%) in group 3. Overall, SARS-CoV-2 PCR tests on 5306 SAL samples and 2896 RAgTs were performed in children, with 1 asymptomatic child detected by PCR from SAL. Successful long-term participation was highest in group 2 (SAL only; children: 111 of 172 [64.5%]; CCWs: 18 of 29 [62.1%]). Weekly participation rates in children ranged from 54.0% to 83.8% for SAL and from 44.6% to 61.4% for RAgT. Participation rates decreased during the study course (P < .001). The probability of SARS-CoV-2 introduction into a DCC with 50 children was estimated to reach at most 5% for an age-adjusted SARS-CoV-2 incidence below 143.
Conclusions and relevance: Self-sampling for continuous SARS-CoV-2 testing was well accepted, with SAL being the preferred method. Given the high number of negative tests, thresholds for initiating continuous testing should be established based on age-adjusted SARS-CoV-2 incidence rates.
Trial registration: German Registry for Clinical Trials Identifier: DRKS00025546.
Conflict of interest statement
Figures
References
-
- Sorg A, Hufnagel M, Doenhardt M, et al. Risk of hospitalization, severe disease, and mortality due to COVID-19 and PIMS-TS in children with SARS-CoV-2 infection in Germany. medRxiv. Preprint posted online November 30, 2021. doi: 10.1101/2021.11.30.21267048 - DOI
-
- Wang L, Berger NA, Kaelber DC, Davis PB, Volkow ND, Xu R. COVID infection severity in children under 5 years old before and after Omicron emergence in the US. medRxiv. Preprint posted online January 13, 2022. doi: 10.1101/2022.01.12.22269179 - DOI
-
- Walger P, Heininger U, Knuf M, et al. Kinder und Jugendliche in der Covid-19-Pandemie: Schulen und Kitas sollen wieder geöffnet werden. Der Schutz von Lehrern, Erziehern, Betreuern und Eltern und die allgemeinen Hygieneregeln stehen dem nicht entgegen. Accessed August 15, 2022. https://dgpi.de/stellungnahme-schulen-und-kitas-sollen-wieder-geoeffnet-...
-
- Lachassinne E, de Pontual L, Caseris M, et al. ; COVIDOCRECHE collaborators . SARS-CoV-2 transmission among children and staff in daycare centres during a nationwide lockdown in France: a cross-sectional, multicentre, seroprevalence study. Lancet Child Adolesc Health. 2021;5(4):256-264. doi: 10.1016/S2352-4642(21)00024-9 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
