

Bypassing the post-anaesthesia care unit after elective hip and knee arthroplasty: a prospective cohort safety study
- PMID: 36108163
- PMCID: PMC10086992
- DOI: 10.1111/anae.15852
Bypassing the post-anaesthesia care unit after elective hip and knee arthroplasty: a prospective cohort safety study
Erratum in
-
Correction to "Bypassing the post-anaesthesia care unit after elective hip and knee arthroplasty: a prospective cohort safety study".Anaesthesia. 2023 May;78(5):663. doi: 10.1111/anae.15998. Anaesthesia. 2023. PMID: 37015748 Free PMC article. No abstract available.
Abstract
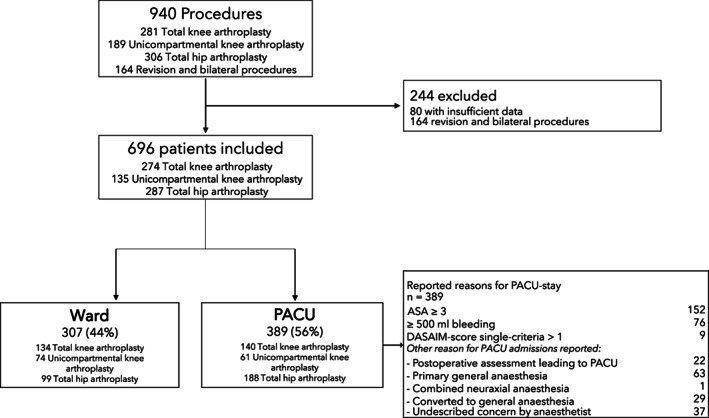
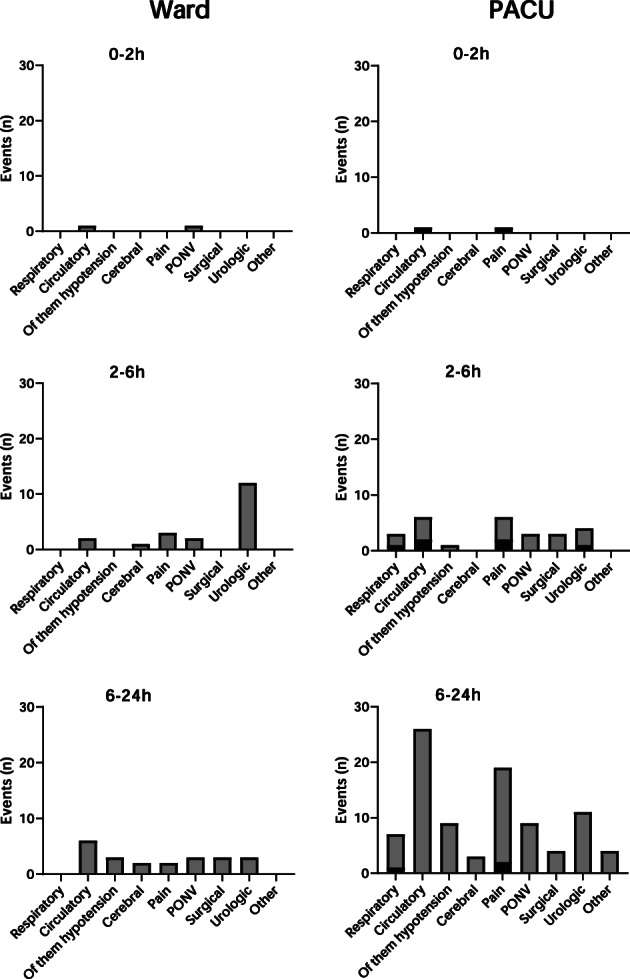
Following knee and hip arthroplasty, transfer to a recovery area immediately following surgery and before going to ward might be unnecessary in low-risk patients. Avoiding the recovery area in this way could allow for more targeted use of resources for higher risk patients, which may improve operating theatre flow and productivity. A prospective single-centre cohort study on the safety of criteria for bypassing the post-anaesthesia care unit in elective hip and knee arthroplasty was designed. Criteria were: ASA physical status < 3; peri-operative bleeding < 500 ml; low postoperative discharge-score (modified Aldrete-score); and an uncomplicated surgical and neuraxial anaesthesia procedure. The primary outcome was the number of patients in need of secondary readmission to the post-anaesthesia care unit. Events within the first 24 postoperative hours were recorded, along with readmission and complication rates. A total of 696 patients were included, with 287 (41%) undergoing total hip arthroplasty, 274 (39%) undergoing total knee arthroplasty and 135 (19%) undergoing unicompartmental knee-arthroplasty. Of these, 207 (44%) bypassed the post-anaesthesia care unit. Patients all received multimodal analgesia without peripheral nerve blockade. Only one patient in the ward group required secondary readmission to the post-anaesthesia care unit. Within 24 h, 151 events were reported, with 41 (27%) in the ward group and 110 (73%) in the post-anaesthesia care unit group. Two events in each group occurred within 2 hours of surgery. No complications were attributed to bypassing the post-anaesthesia care unit. The use of simple pragmatic criteria for bypassing the post-anaesthesia care unit for patients undergoing knee and hip arthroplasty with spinal anaesthesia is possible and associated with significant reduction of post-anaesthesia care unit admission and without apparent safety issues. Confirmation is needed from other studies and external validity should be interpreted cautiously in centres with different peri-operative regimens, organisational and staffing structures.
Keywords: PACU; enhanced recovery; hip arthroplasty; knee arthroplasty.
© 2022 The Authors. Anaesthesia published by John Wiley & Sons Ltd on behalf of Association of Anaesthetists.
Figures
Comment in
-
Turning baby steps into big leaps: shifting paradigms in fast-track joint replacement surgery.Anaesthesia. 2023 Jan;78(1):14-16. doi: 10.1111/anae.15903. Epub 2022 Oct 28. Anaesthesia. 2023. PMID: 36308017 No abstract available.
-
Bypassing the post-anaesthesia care unit after elective hip and knee arthroplasty.Anaesthesia. 2023 Jun;78(6):786-787. doi: 10.1111/anae.15992. Epub 2023 Feb 21. Anaesthesia. 2023. PMID: 36802276 No abstract available.
-
Bypassing the post-anaesthesia care unit after elective hip and knee arthroplasty.Anaesthesia. 2023 Jun;78(6):788-789. doi: 10.1111/anae.16003. Epub 2023 Mar 21. Anaesthesia. 2023. PMID: 36942829 No abstract available.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
