

Combined nivolumab and ipilimumab with or without stereotactic body radiation therapy for advanced Merkel cell carcinoma: a randomised, open label, phase 2 trial
- PMID: 36108657
- PMCID: PMC9533323
- DOI: 10.1016/S0140-6736(22)01659-2
Combined nivolumab and ipilimumab with or without stereotactic body radiation therapy for advanced Merkel cell carcinoma: a randomised, open label, phase 2 trial
Abstract
Background: Merkel cell carcinoma is among the most aggressive and lethal of primary skin cancers, with a high rate of distant metastasis. Anti-programmed death receptor 1 (anti-PD-1) and programmed death ligand 1 (PD-L1) monotherapy is currently standard of care for unresectable, recurrent, or metastatic Merkel cell carcinoma. We assessed treatment with combined nivolumab plus ipilimumab, with or without stereotactic body radiotherapy (SBRT) in patients with advanced Merkel cell carcinoma as a first-line therapy or following previous treatment with anti-PD-1 and PD-L1 monotherapy.
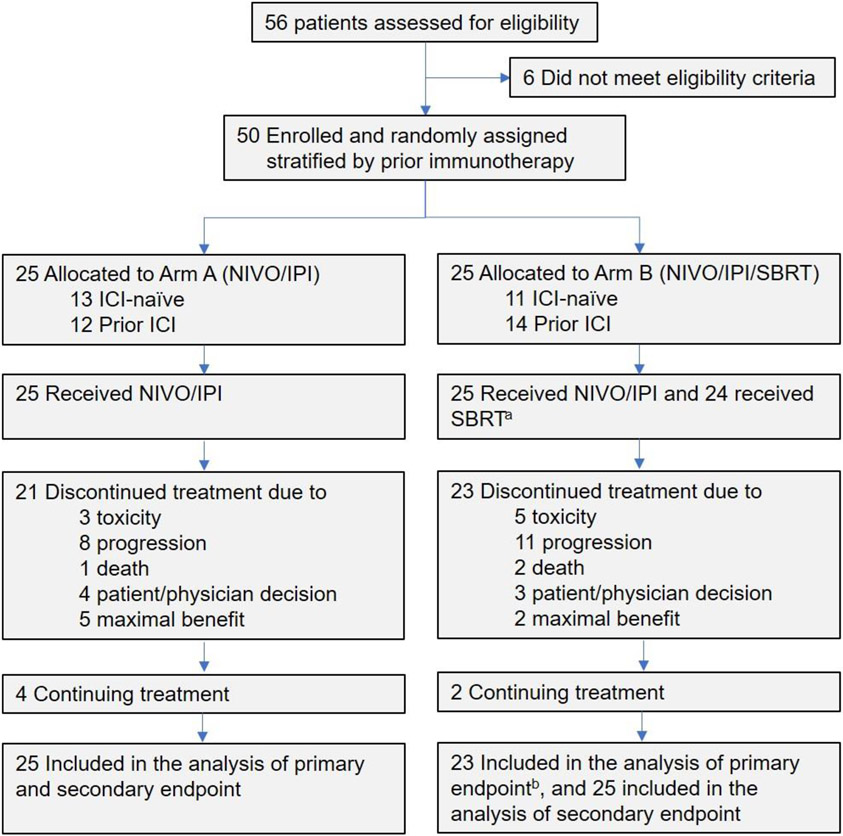
Methods: In this randomised, open label, phase 2 trial, we randomly assigned adults from two cancer sites in the USA (one in Florida and one in Ohio) to group A (combined nivolumab and ipilimumab) or group B (combined nivolumab and ipilimumab plus SBRT) in a 1:1 ratio. Eligible patients were aged at least 18 years with histologically proven advanced stage (unresectable, recurrent, or stage IV) Merkel cell carcinoma, a minimum of two tumour lesions measureable by CT, MRI or clinical exam, and tumour tissue available for exploratory biomarker analysis. Patients were stratified by previous immune-checkpoint inhibitor (ICI) status to receive nivolumab 240 mg intravenously every 2 weeks plus ipilimumab 1 mg/kg intravenously every 6 weeks (group A) or the same schedule of combined nivolumab and ipilimumab with the addition of SBRT to at least one tumour site (24 Gy in three fractions at week 2; group B). Patients had to have at least two measurable sites of disease so one non-irradiated site could be followed for response. The primary endpoint was objective response rate (ORR) in all randomly assigned patients who received at least one dose of combined nivolumab and ipilimumab. ORR was defined as the proportion of patients with a complete response or partial response per immune-related Response Evaluation Criteria in Solid Tumours. Response was assessed every 12 weeks. Safety was assessed in all patients. This trial is registered with ClinicalTrials.gov, NCT03071406.
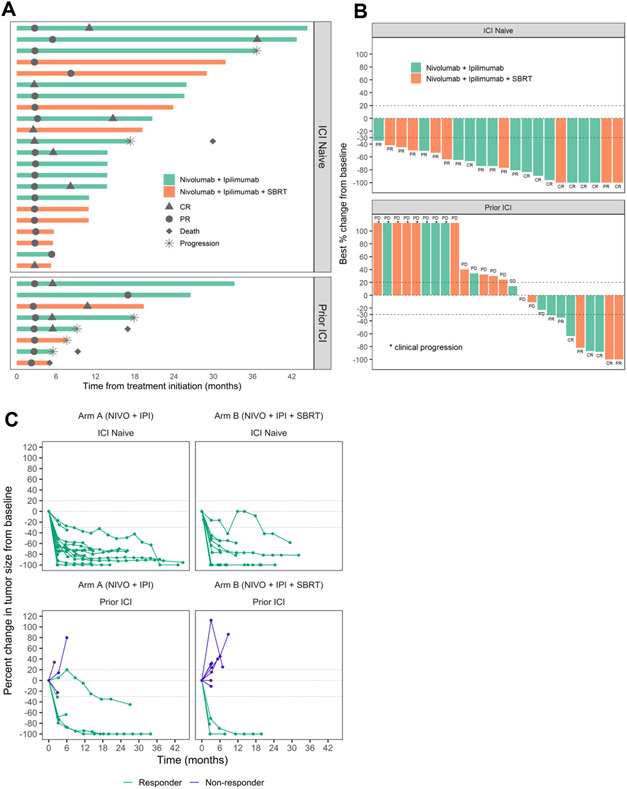
Findings: 50 patients (25 in both group A and group B) were enrolled between March 14, 2017, and Dec 21, 2021, including 24 ICI-naive patients (13 [52%] of 25 group A patients and 11 [44%] of 25 group B patients]) and 26 patients with previous ICI (12 [48%] of 25 group A patients and 14 [56%] of 25 group B patients]). One patient in group B did not receive SBRT due to concerns about excess toxicity. Median follow-up was 14·6 months (IQR 9·1-26·5). Two patients in group B were excluded from the analysis of the primary endpoint because the target lesions were irradiated and so the patients were deemed non-evaluable. Of the ICI-naive patients, 22 (100%) of 22 (95% CI 82-100) had an objective response, including nine (41% [95% CI 21-63]) with complete response. Of the patients who had previously had ICI exposure, eight (31%) of 26 patients (95% CI 15-52) had an objective response and four (15% [5-36]) had a complete response. No significant differences in ORR were observed between groups A (18 [72%] of 25 patients) and B (12 [52%] of 23 patients; p=0·26). Grade 3 or 4 treatment-related adverse events were observed in 10 (40%) of 25 patients in group A and 8 (32%) of 25 patients in group B.
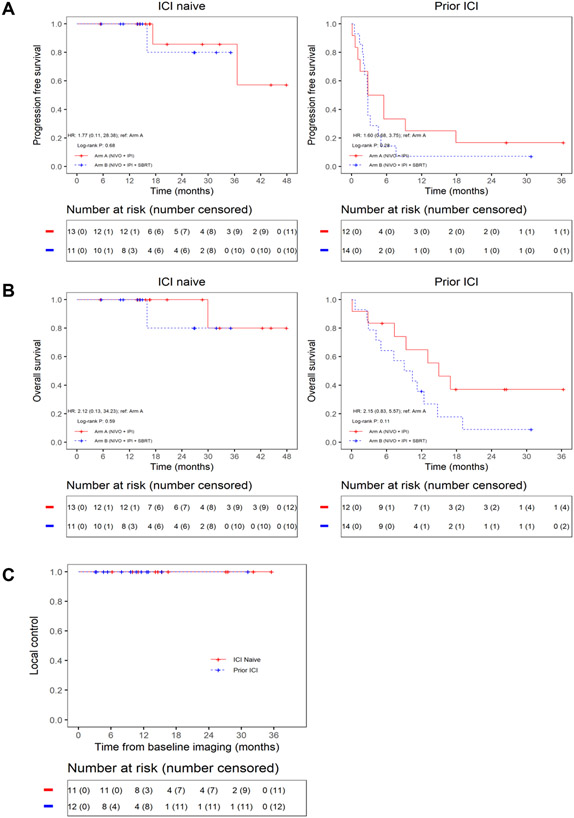
Interpretation: First-line combined nivolumab and ipilimumab in patients with advanced Merkel cell carcinoma showed a high ORR with durable responses and an expected safety profile. Combined nivolumab and ipilimumab also showed clinical benefit in patients with previous anti-PD-1 and PD-L1 treatment. Addition of SBRT did not improve efficacy of combined nivolumab and ipilimumab. The combination of nivolumab and ipilimumab represents a new first-line and salvage therapeutic option for advanced Merkel cell carcinoma.
Funding: Bristol Myers Squibb Rare Population Malignancy Program.
Copyright © 2022 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Declaration of interests SK reports research support from Bristol Myers Squibb for the submitted work and research support from Bristol Myers Squibb and AstraZeneca outside the submitted work. EW reports being a member of the advisory board for Viewray, Varian, Alphatau, Castle Biosciences, and Teiko outside the submitted work. ZE reports being a member of the advisory board for Array, Pfizer, OncoSec, Regeneron, Genentech, Novartis, Natera, and Eisai outside the submitted work and research support for Novartis, Pfizer, and Boehringer-Ingelheim outside the submitted work. JJC reports research support for Varian and Galera outside the submitted work. AT reports research support for Bristol Myers Squibb, Genentech-Roche, Regeneron, Sanofi-Genzyme, Nektar, Clinigen, Merck, Acrotech, Pfizer, Checkmate, and OncoSec outside the submitted work and personal fees from Bristol Myers Squibb, Merck, Eisai, Instil Bio, Clinigen, Regeneron, Sanofi-Genzyme, Novartis, Partner Therapeutics, Genentech/Roche, and BioNTech outside the submitted work. JM reports research support from Microba, Jackson Laboratories, Merck, and Morphogenesis outside the submitted work. BAP reports being a member of the advisory board for Bristol Myers Squibb, AstraZeneca, and G1 therapeutics outside the submitted work. VKS reports research support from Neogene and Turnstone outside the submitted work and being a member of the advisory board for Bristol Myers Squibb, Eisai, Iovance, Merck, Novartis, Regeneron, and Statking outside the submitted work. NIK reports being a member of the advisory board for Bristol Myers-Squibb, Regeneron, Merck, Jounce Therapeutics, Iovance Biotherapeutics, Genzyme, Novartis, Castle Biosciences, Nektar, and Instill Bio outside the submitted work; being a member of the steering or scientific committee for Nektar, Regeneron, Replimune, Bristol Myers-Squibb, and National Comprehensive Cancer Network via Pfizer outside the submitted work; being on the data safety monitoring committee for AstraZeneca and Incyte outside the submitted work; research support to his institution outside the submitted work from Bristol Myers-Squibb, Merck, Celgene, Regeneron, Replimune, Novartis, HUYA Bioscience, and GlaxoSmithKline); and common stock from Bellicum, Amarin, Asensus Surgical outside the submitted work. ASB reports being a member of the advisory board for Deciphera and Bayer outside the submitted work. All other authors have no interests to declare.
Figures
Comment in
-
Combined nivolumab and ipilimumab in non-resectable Merkel cell carcinoma.Lancet. 2022 Sep 24;400(10357):976-977. doi: 10.1016/S0140-6736(22)01749-4. Epub 2022 Sep 12. Lancet. 2022. PMID: 36108656 No abstract available.
References
-
- Schadendorf D, Lebbe C, Zur Hausen A, et al. Merkel cell carcinoma: Epidemiology, prognosis, therapy and unmet medical needs. European journal of cancer 2017; 71: 53–69. - PubMed
-
- Knepper TC, Montesion M, Russell JS, et al. The Genomic Landscape of Merkel Cell Carcinoma and Clinicogenomic Biomarkers of Response to Immune Checkpoint Inhibitor Therapy. Clinical cancer research : an official journal of the American Association for Cancer Research 2019; 25(19): 5961–71. - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
