

Human intestinal myofibroblasts deposited collagen VI enhances adhesiveness for T cells - A novel mechanism for maintenance of intestinal inflammation
- PMID: 36108990
- PMCID: PMC10043923
- DOI: 10.1016/j.matbio.2022.09.001
Human intestinal myofibroblasts deposited collagen VI enhances adhesiveness for T cells - A novel mechanism for maintenance of intestinal inflammation
Abstract
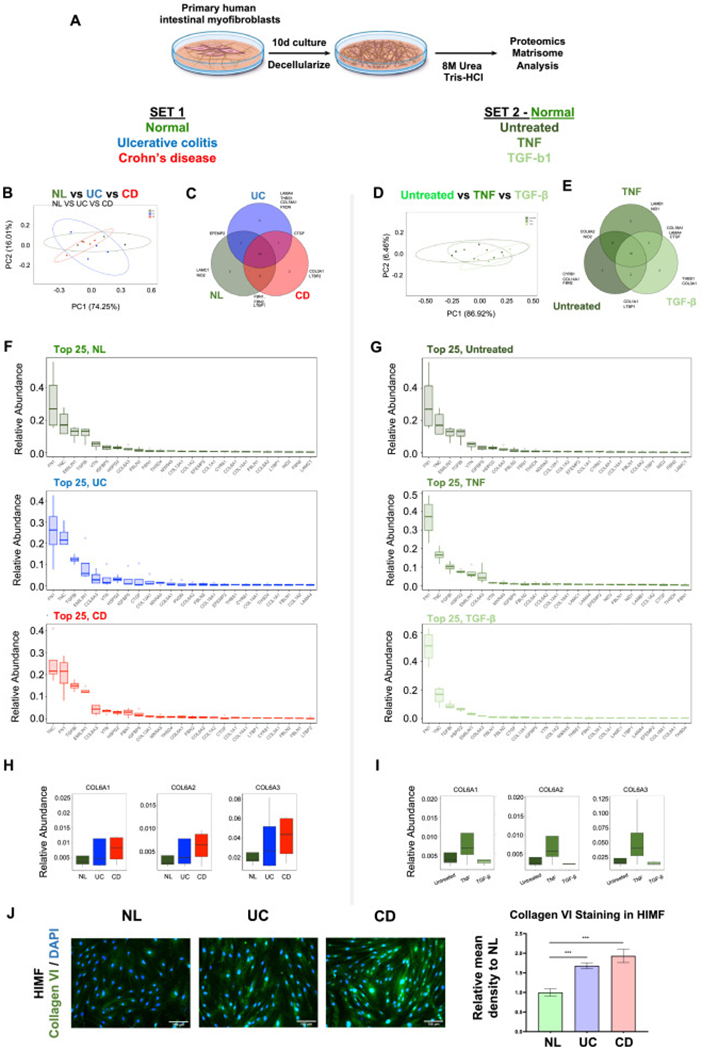
Objective: Inflammatory bowel diseases (IBD) cause chronic intestinal damage and extracellular matrix (ECM) remodeling. The ECM may play an active role in inflammation by modulating immune cell functions, including cell adhesion, but this hypothesis has not been tested in IBD.
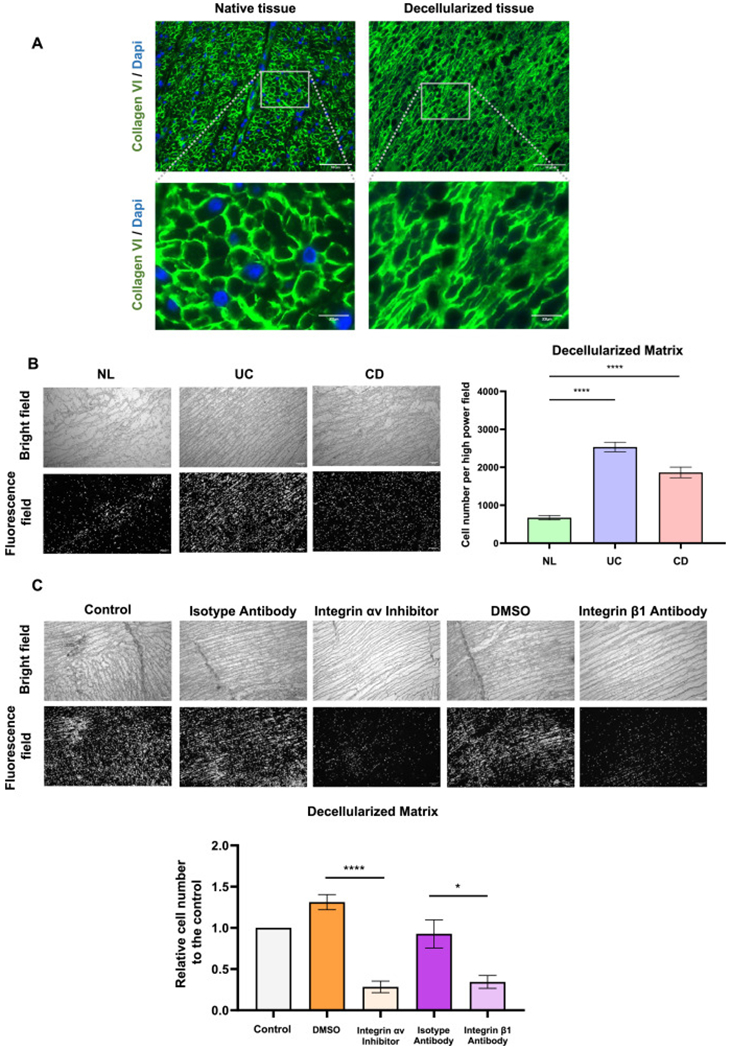
Design: Primary human intestinal myofibroblast (HIMF)-derived ECM from IBD and controls, 3D decellularized colon or ECM molecule-coated scaffolds were tested for their adhesiveness for T cells. Matrisome was analysed via proteomics. Functional integrin blockade was used to investigate the underlying mechanism. Analysis of the pediatric Crohn's disease (CD) RISK inception cohort was used to explore an altered ECM gene expression as a potential predictor for a future complicated disease course.
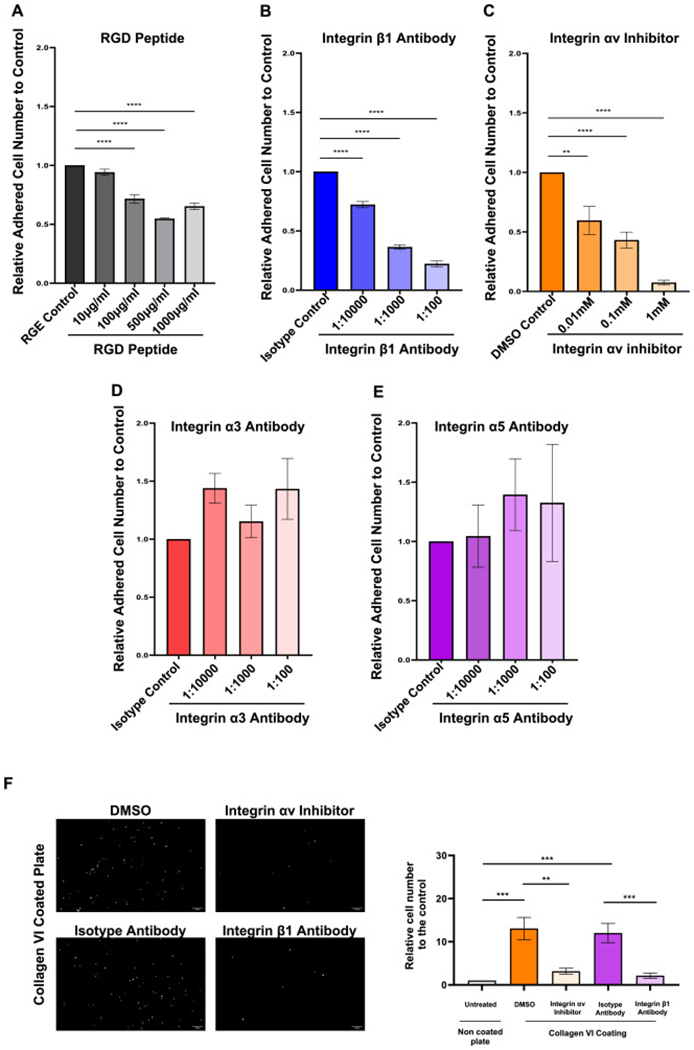
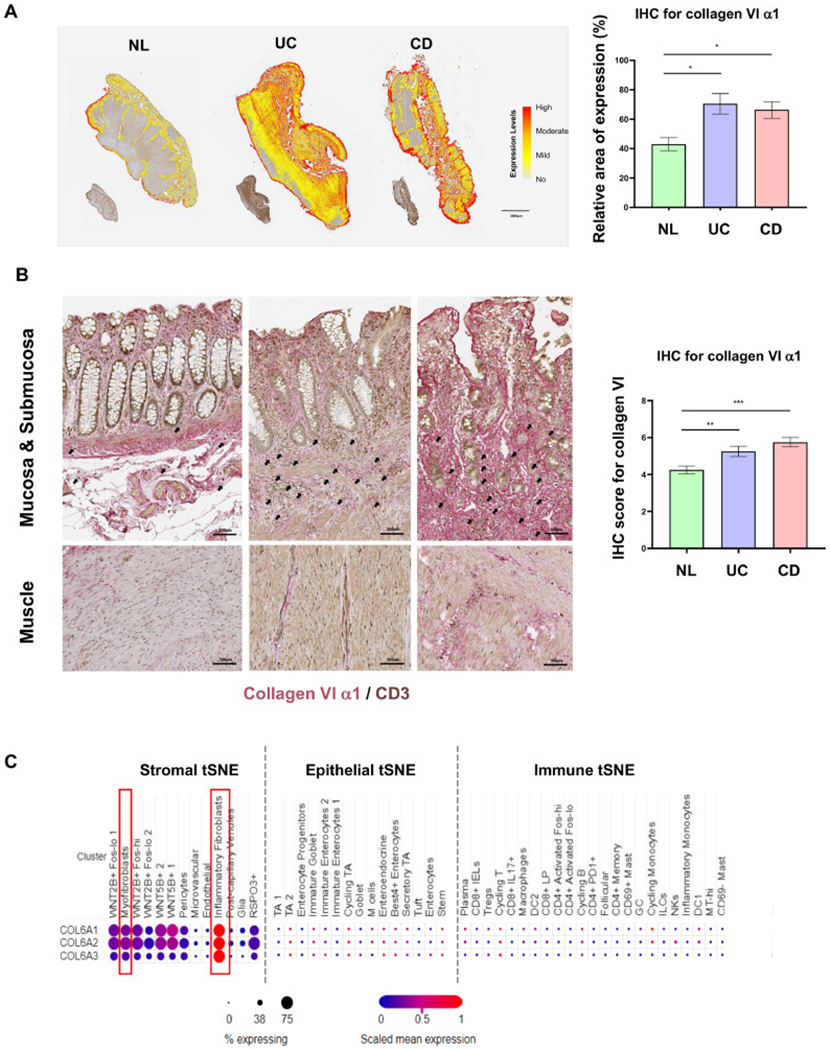
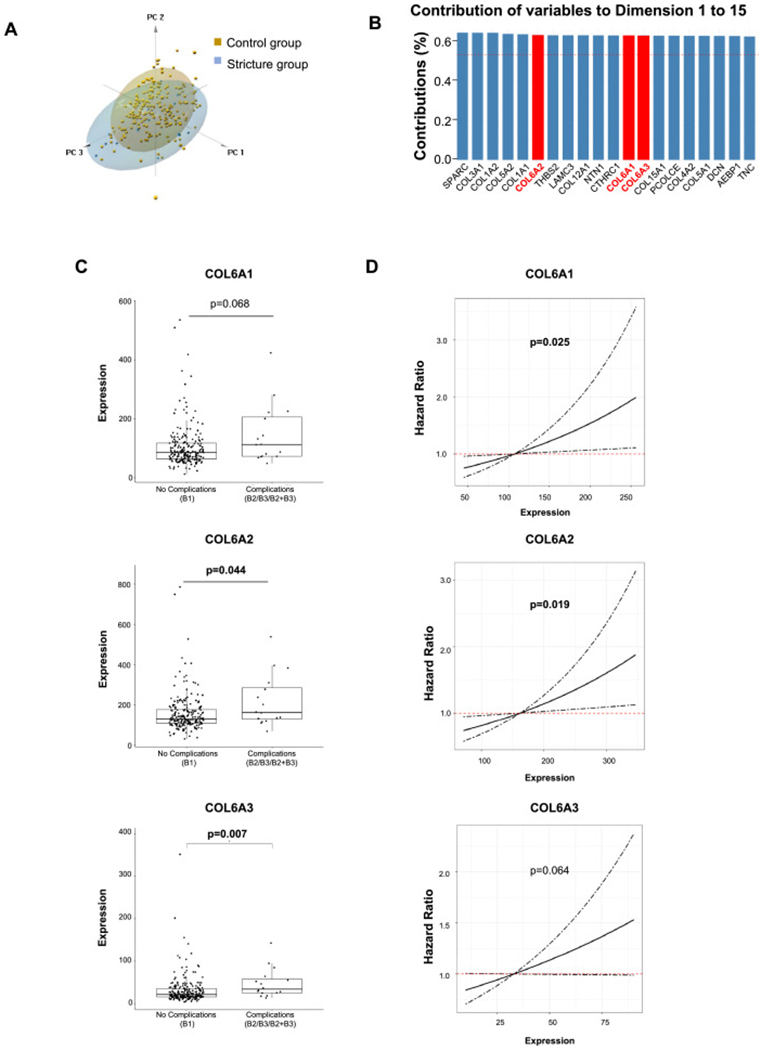
Results: HIMF-derived ECM and 3D decellularized colonic ECM from IBD bound more T cells compared to control. Control HIMFs exposed to the pro-inflammatory cytokines Iinterleukin-1β (IL-1β) and tumor necrosis factor (TNF) increased, and to transforming growth factor-β1 (TGF-β1) decreased ECM adhesiveness to T cells. Matrisome analysis of the HIMF-derived ECM revealed collagen VI as a major culprit for differences in T cell adhesion. Collagen VI knockdown in HIMF reduced adhesion T cell as did the blockage of integrin αvβ1. Elevated gene expression of collagen VI in biopsies of pediatric CD patients was linked to risk for future stricturing disease.
Conclusion: HIMF-derived ECM in IBD binds a remarkably enhanced number of T cells, which is dependent on Collagen VI and integrin αvβ1. Collagen VI expression is a risk factor for a future complicated CD course. Blocking immune cells retention may represent a novel approach to treatment in IBD.
Keywords: Cell adhesion; Extracellular matrix; Inflammatory bowel disease; Intestinal T cells.
Copyright © 2022. Published by Elsevier B.V.
Conflict of interest statement
Declaration of Competing Interest F.R. is consultant to Agomab, Allergan, AbbVie, Boehringer-Ingelheim, Celgene, Cowen, Genentech, Gilead, Gossamer, Guidepoint, Helmsley, Index Pharma, Jannsen, Koutif, Metacrine, Morphic, Pfizer, Pliant, Prometheus Biosciences, Receptos, RedX, Roche, Samsung, Takeda, Techlab, Thetis, UCB, 89Bio. C.F. received speaker fees from UCB, Genentech, Sandoz, Janssen and he is consultant for Athos Therapeutics, Inc.
Figures


References
-
- Mortensen JH, Lindholm M, Langholm LL, Kjeldsen J, Bay-Jensen AC, Karsdal MA, Manon-Jensen T, The intestinal tissue homeostasis - the role of extracellular matrix remodeling in inflammatory bowel disease, Expert Rev. Gastroenterol. Hepatol 13 (10) (2019) 977–993. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
