

Biopsy and blood-based molecular biomarker of inflammation in IBD
- PMID: 36109152
- PMCID: PMC10014487
- DOI: 10.1136/gutjnl-2021-326451
Biopsy and blood-based molecular biomarker of inflammation in IBD
Abstract
Objective: IBD therapies and treatments are evolving to deeper levels of remission. Molecular measures of disease may augment current endpoints including the potential for less invasive assessments.
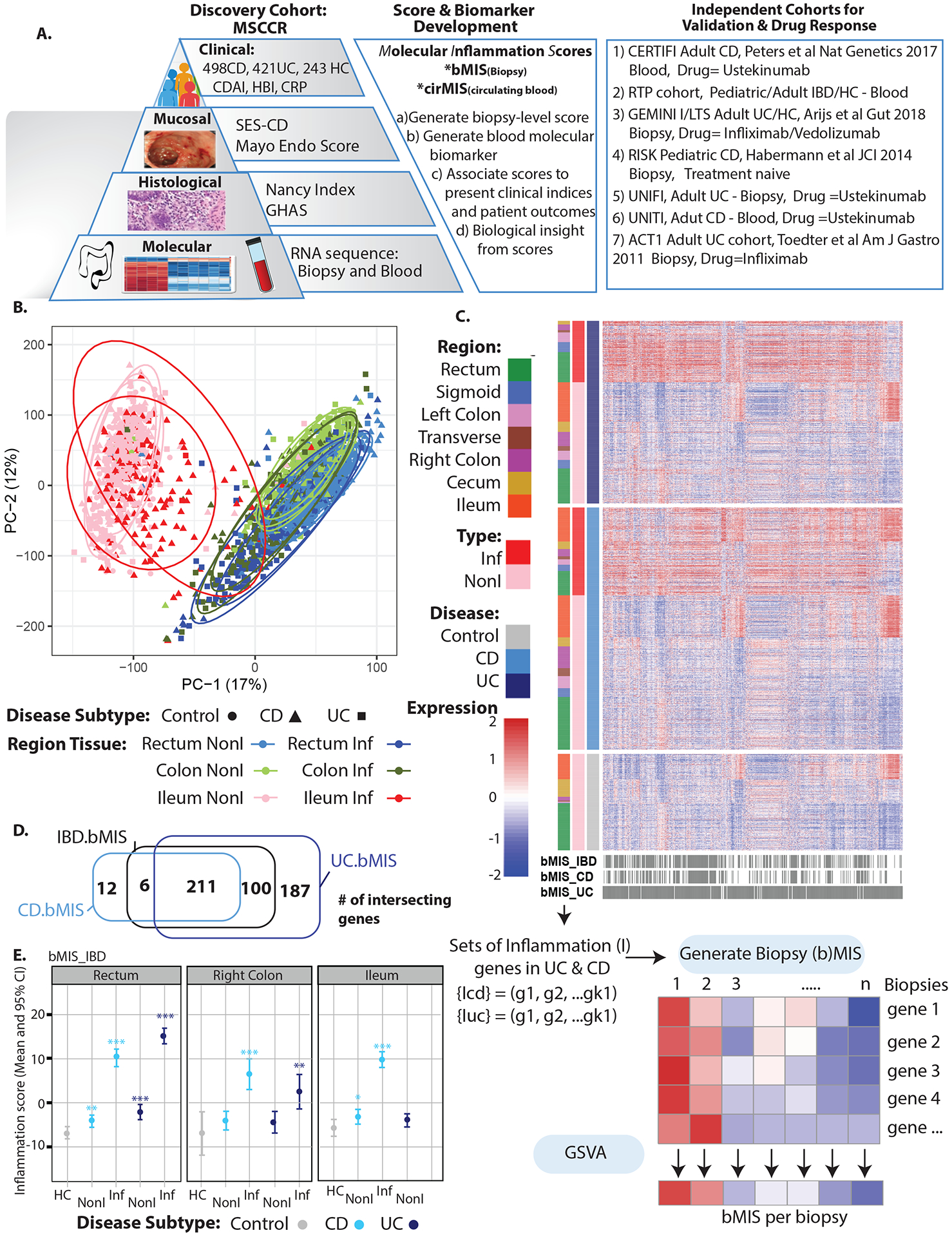
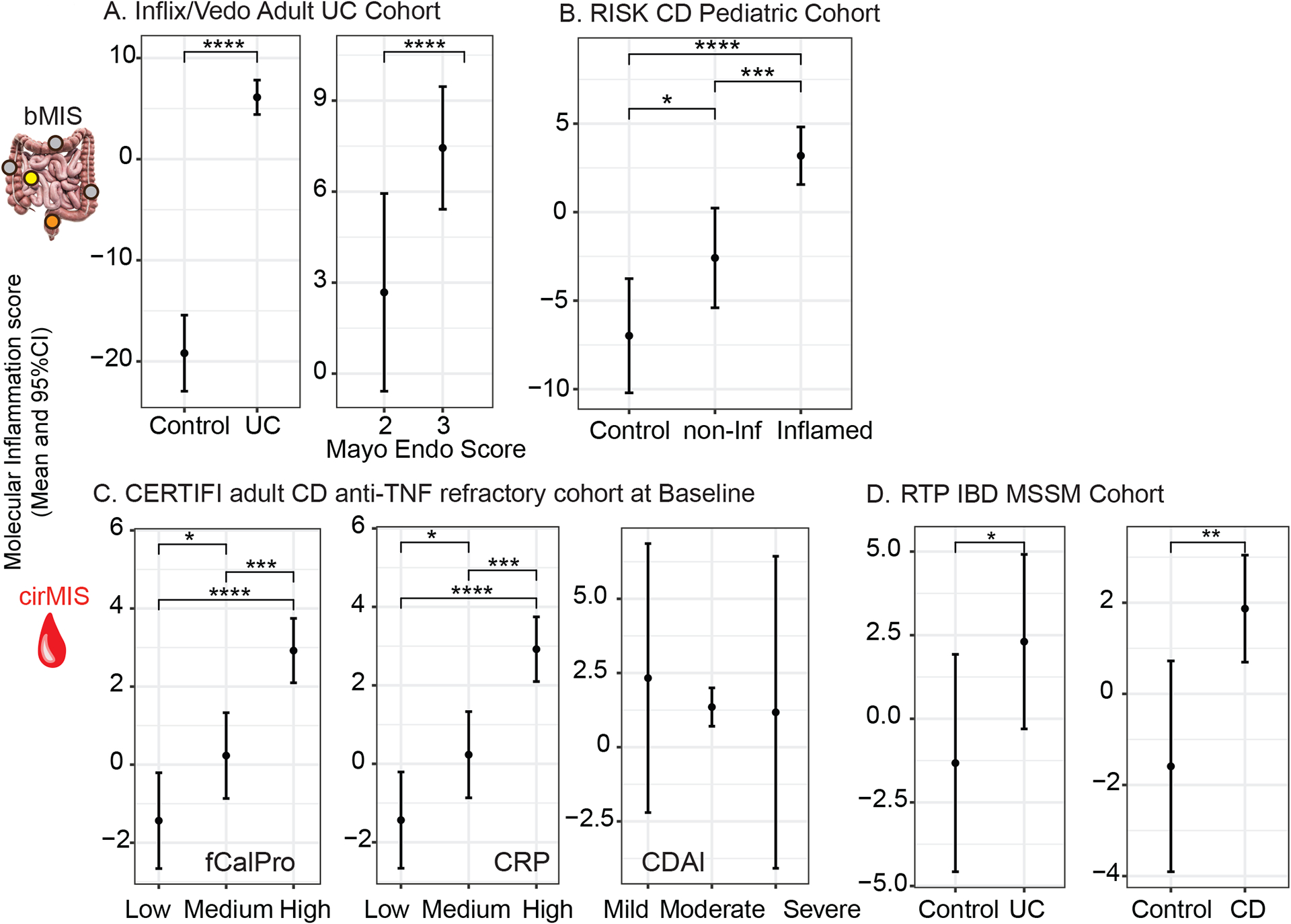
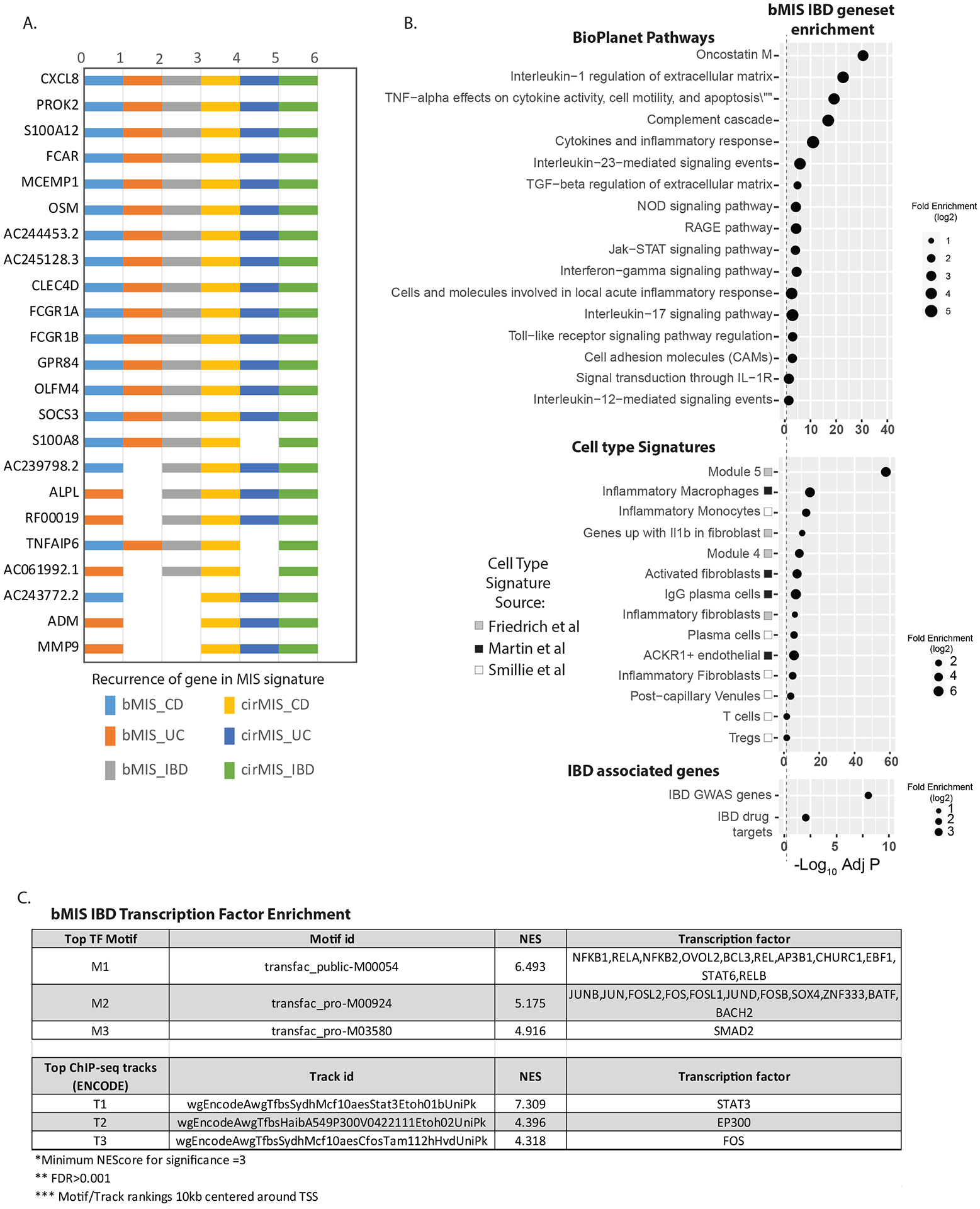
Design: Transcriptome analysis on 712 endoscopically defined inflamed (Inf) and 1778 non-inflamed (Non-Inf) intestinal biopsies (n=498 Crohn's disease, n=421 UC and 243 controls) in the Mount Sinai Crohn's and Colitis Registry were used to identify genes differentially expressed between Inf and Non-Inf biopsies and to generate a molecular inflammation score (bMIS) via gene set variance analysis. A circulating MIS (cirMIS) score, reflecting intestinal molecular inflammation, was generated using blood transcriptome data. bMIS/cirMIS was validated as indicators of intestinal inflammation in four independent IBD cohorts.
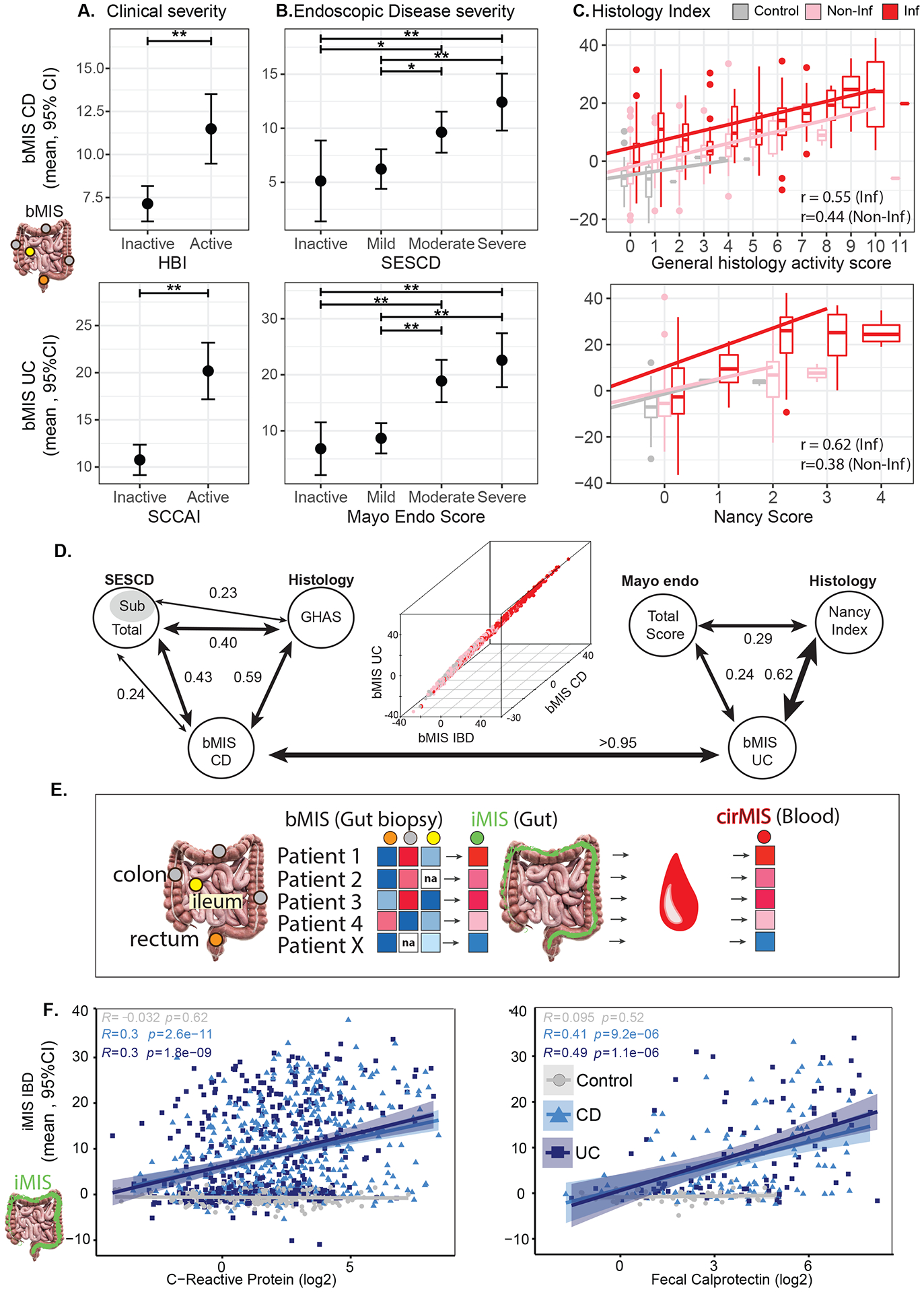
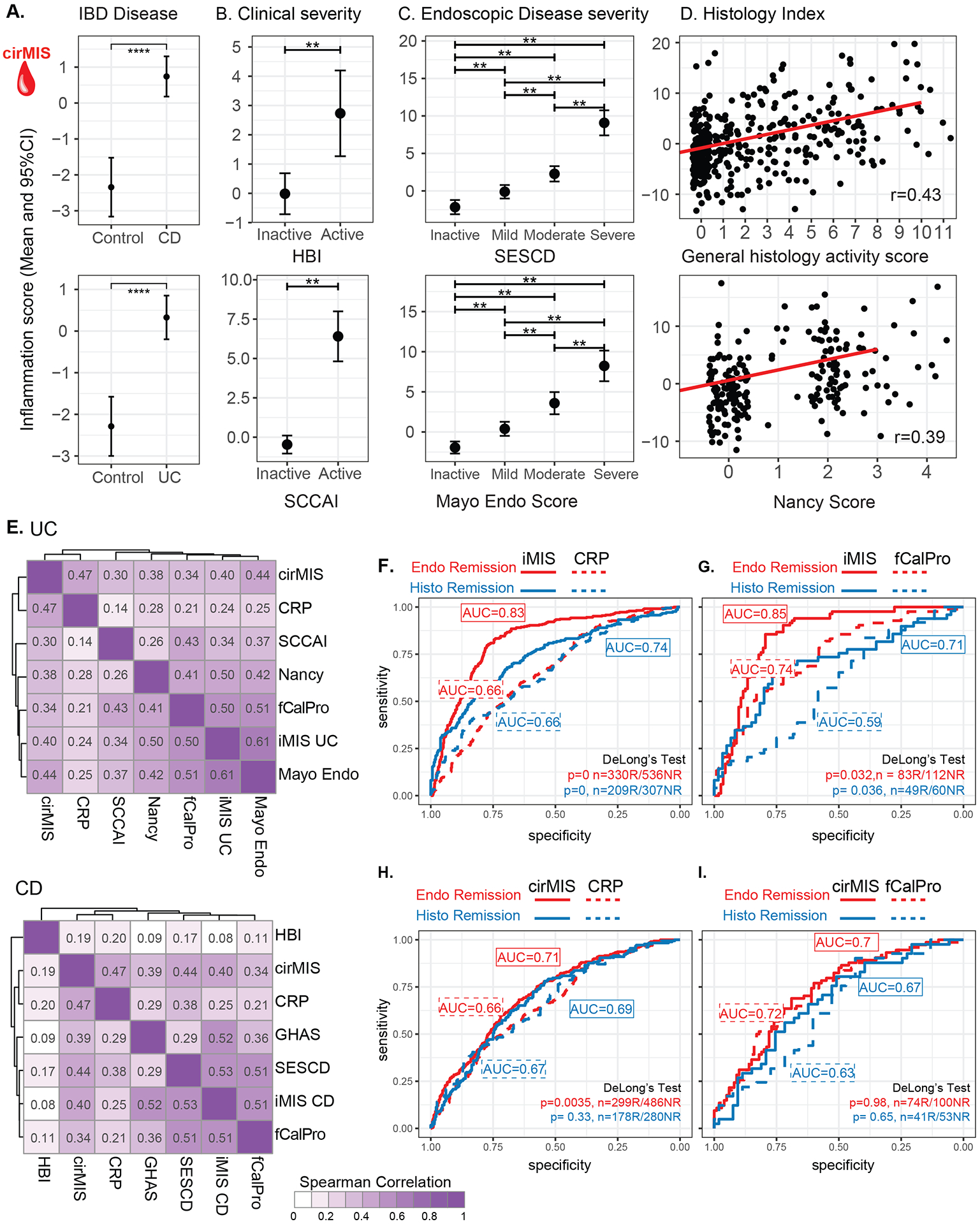
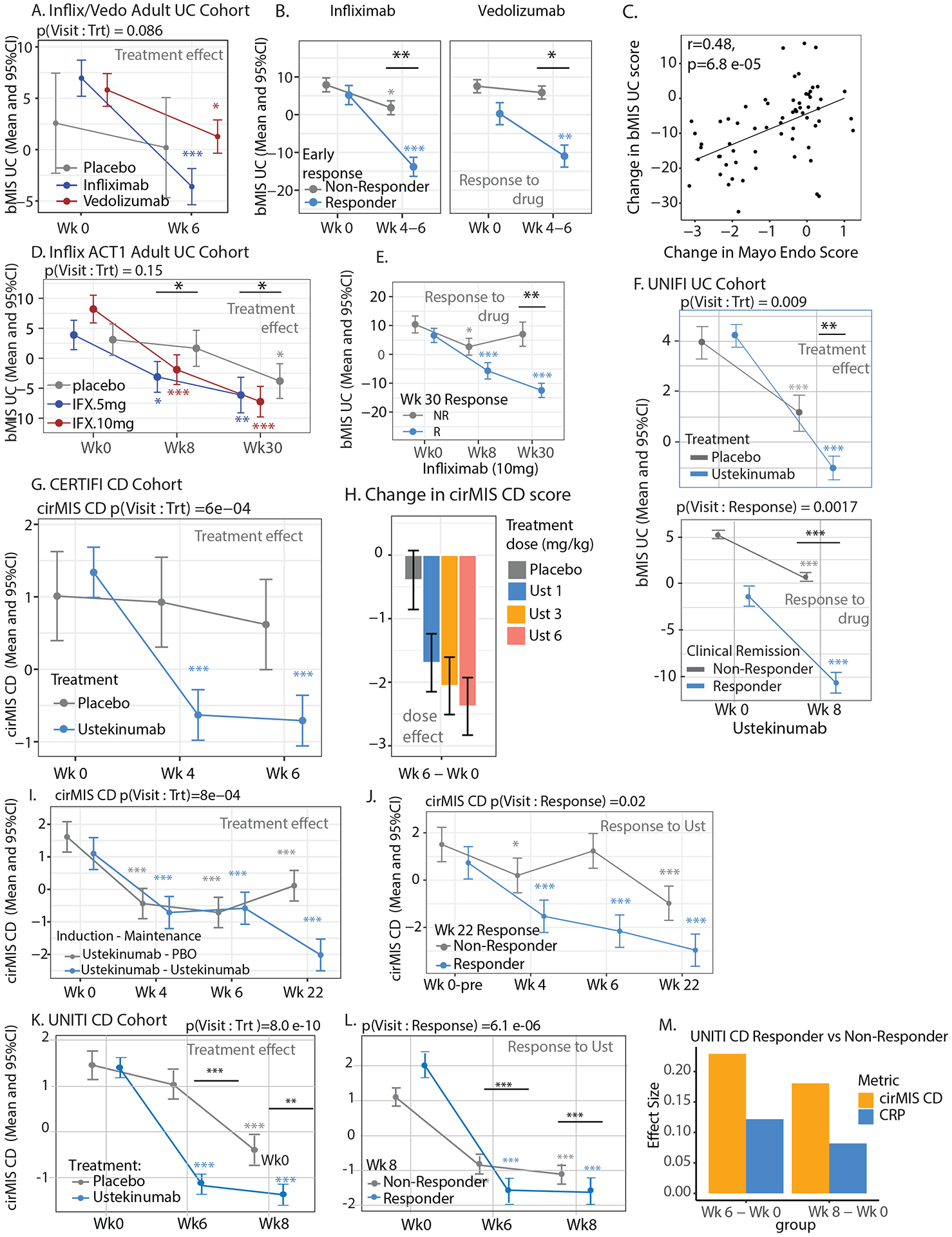
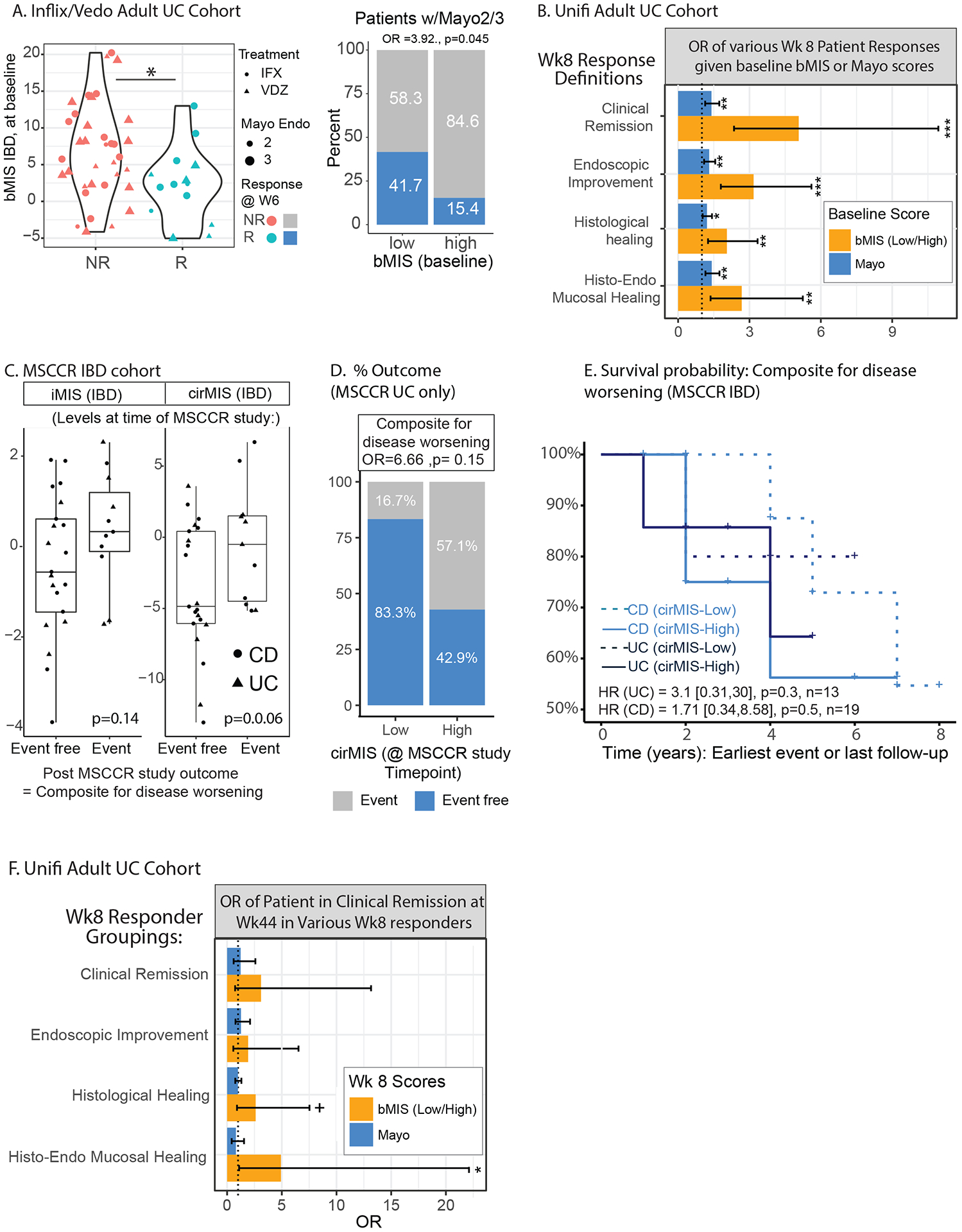
Results: bMIS/cirMIS was strongly associated with clinical, endoscopic and histological disease activity indices. Patients with the same histologic score of inflammation had variable bMIS scores, indicating that bMIS describes a deeper range of inflammation. In available clinical trial data sets, both scores were responsive to IBD treatment. Despite similar baseline endoscopic and histologic activity, UC patients with lower baseline bMIS levels were more likely treatment responders compared with those with higher levels. Finally, among patients with UC in endoscopic and histologic remission, those with lower bMIS levels were less likely to have a disease flare over time.
Conclusion: Transcriptionally based scores provide an alternative objective and deeper quantification of intestinal inflammation, which could augment current clinical assessments used for disease monitoring and have potential for predicting therapeutic response and patients at higher risk of disease flares.
Keywords: IBD; IBD CLINICAL; MOLECULAR MECHANISMS; MOLECULAR PATHOLOGY; STATISTICS.
© Author(s) (or their employer(s)) 2023. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: Mount Sinai co-authors (from Genetics and Genomics, Icahn Institute for Data Science and Genomic Technology, Population Health Science and Policy, Division of Gastroenterology, Pediatric GI and Hepatology, Susan and Leonard Feinstein IBD Clinical Center at Icahn School of Medicine at Mount Sinai) were partially funded as part of research alliance between Janssen Biotech and The Icahn School of Medicine at Mount Sinai. SV, PTD, PB, AS, JP, CB, MC, EL-S and JW are employees at Janssen Biotech, Inc. Joshua R. Friedman is a former employee at Janssen Biotech, Inc. KH, MM, AK, AD and ES are employees at Sema4. BS, J-FC and MCD are consultants for Janssen. MCD is an advisory board member of Janssen.RCU has served as an advisory board member or consultant for AbbVie, Bristol Myers Squibb, Janssen, Pfizer, and Takeda; research support from AbbVie, Boehringer Ingelheim, Eli Lilly, and Pfizer.B.E.S. discloses the following: consulting fees from 4D Pharma, Abbvie, Allergan, Amgen, Arena Pharmaceuticals, AstraZeneca, Boehringer Ingelheim, Boston Pharmaceuticals, Capella Biosciences, Celgene, Celltrion Healthcare, EnGene, Ferring, Genentech, Gilead, Hoffmann-La Roche, Immunic, Ironwood Pharmaceuticals, Janssen, Lilly, Lyndra, MedImmune, Morphic Therapeutic, Oppilan Pharma, OSE Immunotherapeutics, Otsuka, Palatin Technologies, Pfizer, Progenity, Prometheus Laboratories, Redhill Biopharma, Rheos Medicines, Seres Therapeutics, Shire, Synergy Pharmaceuticals, Takeda, Target PharmaSolutions, Theravance Biopharma R&D, TiGenix, and Vivelix Pharmaceuticals; honoraria for speaking in CME programs from Takeda, Janssen, Lilly, Gilead, Pfizer, and Genetech; and research funding from Celgene, Pfizer, Takeda, Theravance Biopharma R&D, and Janssen.M.C.D. discloses consulting fees from Abbvie, Allergan, Amgen, Arena Pharmaceuticals, AstraZeneca, Boehringer Ingelheim, Celgene, Ferring, Genentech, Gilead, Hoffmann-La Roche, Janssen, Pfizer, Prometheus Biosciences, Takeda, and Target PharmaSolutions and research funding from Abbvie, Janssen, Pfizer, and Prometheus Biosciences Takeda.J-F.C. reports: receiving research grants from AbbVie, Janssen Pharmaceuticals, and Takeda; receiving payment for lectures from AbbVie, Amgen, Allergan, Inc., Ferring Pharmaceuticals, Shire, and Takeda; receiving consulting fees from AbbVie, Amgen, Arena Pharmaceuticals, Boehringer Ingelheim, Bristol Myers Squibb, Celgene Corporation, Eli Lilly, Ferring Pharmaceuticals, Galmed Research, Glaxo Smith Kline, Geneva, Iterative Scopes, Janssen Pharmaceuticals, Kaleido Biosciences, Landos, Otsuka, Pfizer, Prometheus, Sanofi, Takeda, and TiGenix; and holding stock options in Intestinal Biotech Development.S.M. has received investigator-initiated grant funding from Takeda Pharma and Genentech and has served as consultant or paid speaker for Takeda Pharma, Genentech, Morphic, and Glaxo Smith Kline. RCU supported by an NIH K23 Career Development Award (K23KD111995-01A1). CA, LP, PHC, GW and ES were supported in part by The Leona M. and Harry B. Helmsley Charitable Trust and LP, ES, CA and PHC also by an RC2 DK122532/DK/NIDDK NIH.
Figures
Comment in
-
Going deeper: molecular inflammatory scores in IBD.Gut. 2023 Jul;72(7):1233-1234. doi: 10.1136/gutjnl-2022-328539. Epub 2022 Oct 28. Gut. 2023. PMID: 36307179 No abstract available.
References
-
- Kobayashi T et al. Ulcerative colitis. Nature Reviews Disease Primers 6, 74 (2020). - PubMed
-
- Roda G et al. Crohn’s disease. Nature Reviews Disease Primers 6, 22 (2020). - PubMed
-
- Peyrin-Biroulet L et al. Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE): Determining Therapeutic Goals for Treat-to-Target. Am J Gastroenterol 110, 1324–38 (2015). - PubMed
-
- Le Berre C, Peyrin-Biroulet L & group S.-I.s. Selecting End Points for Disease-Modification Trials in Inflammatory Bowel Disease: the SPIRIT Consensus From the IOIBD. Gastroenterology 160, 1452–1460 e21 (2021). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases