

Derotational distal femoral osteotomy for patients with recurrent patellar instability and increased femoral antetorsion improves knee function and adequately treats both torsional and valgus malalignment
- PMID: 36109379
- PMCID: PMC10356631
- DOI: 10.1007/s00167-022-07150-9
Derotational distal femoral osteotomy for patients with recurrent patellar instability and increased femoral antetorsion improves knee function and adequately treats both torsional and valgus malalignment
Abstract
Purpose: The aim of the study was to evaluate the functional and radiological outcome following derotational distal femoral osteotomy (D-DFO) in patients with high-grade patellofemoral instability (PFI) and an associated increased femoral antetorsion (FA). It was hypothesized that D-DFO would lead to a good functional and radiological outcome, and that both torsional and coronal malalignment could be normalized.
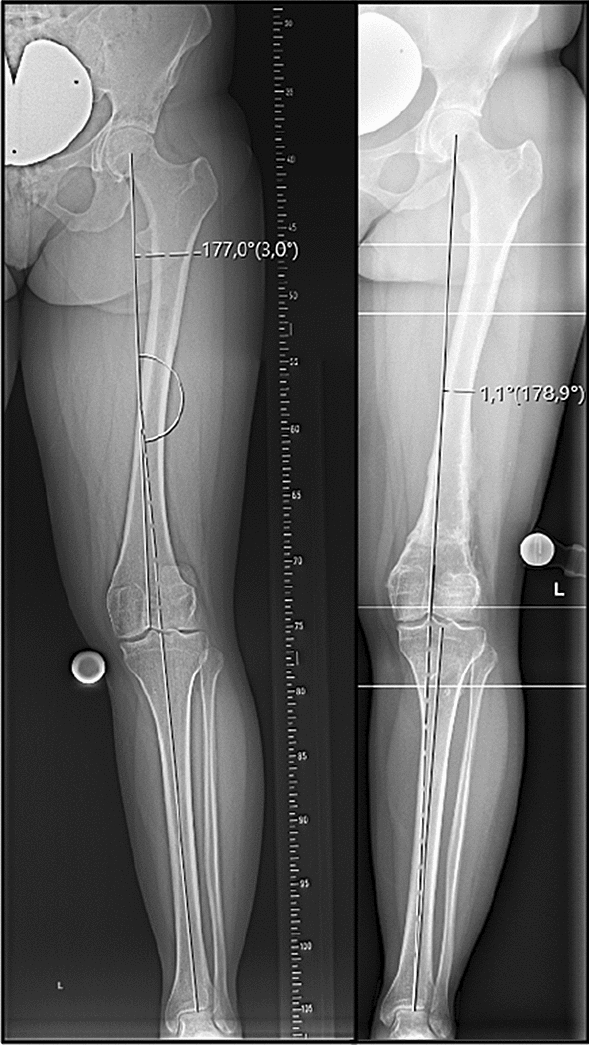
Methods: Patients that underwent D-DFO between 06/2011 and 12/2018 for high-grade PFI with an increased FA (> 20°) were included. Patient-reported outcome measures (Visual Analog Scale [VAS] for pain, Kujala score, Lysholm score, International Knee Documentation Committee subjective knee form [IKDC], and Tegner Activity Scale [TAS]) were evaluated pre- and minimum 24 months postoperatively. Magnetic resonance imaging of the lower extremity and weight-bearing whole-leg anteroposterior radiographs were conducted pre- and postoperatively. The change in FA, coronal limb alignment, and PROMs were tested for statistical significance.
Results: In total, 27 patients (30 knees) were included. The D-DFO aimed to only correct FA (Group 1) or to additionally perform a varization (Group 2) in 14 cases each. In the remaining two cases, double-level osteotomies were performed to correct additional tibial deformities. In 25 cases (83.3%), concomitant procedures also addressing patellofemoral instability were performed. At follow-up (38.0 months [25-75% interquartile range 31.8-52.5 months]), a significant reduction in pain (VAS for pain: 2.0 [1.0-5.0] vs. 0 [0-1.0], p < 0.05), significant improvement in knee function (Kujala Score: 55.6 ± SD 13.6 vs. 80.3 ± 16.7, p < 0.05; Lysholm Score: 58.6 ± 17.4 vs. 79.5 ± 16.6, p < 0.05; IKDC: 54.6 ± 18.7 vs. 74.1 ± 15.0, p < 0.05), and an increase in sporting activity (TAS: 3.0 [3.0-4.0] vs. 4.0 [3.0-5.0], p = n.s.) were reported. Femoral antetorsion was significantly reduced (28.2 ± 6.4° vs. 13.6 ± 5.2°, p < 0.05). A significant varization was observed in Group 2 (2.4 ± 1.2° valgus vs. 0.3 ± 2.4° valgus; p < 0.05). In one case, patellar redislocation occurred 70 months postoperatively.
Conclusion: In patients with PFI and an associated increased FA, D-DFO achieved a significant reduction in pain, an improvement of subjective knee function, as well as an adequate correction of torsional and coronal alignment.
Level of evidence: Retrospective case series, Level IV.
Keywords: Derotational distal femoral osteotomy; Femoral antetorsion; Functional outcome; Patellar dislocation; Patellofemoral instability; Patient-reported outcome measures; Torsional deformity.
© 2022. The Author(s).
Conflict of interest statement
Andreas B. Imhoff is a consultant for Arthrex, Arthrosurface, and Medi Bayreuth, and receives royalties from Arthrex and Arthrosurface.
Figures

References
-
- Deng X, Li L, Zhou P, Deng F, Li Y, He Y, et al. Medial patellofemoral ligament reconstruction combined with biplanar supracondylar femoral derotation osteotomy in recurrent patellar dislocation with increased femoral internal torsion and genu valgum: a retrospective pilot study. BMC Musculoskelet Disord. 2021;22:990. doi: 10.1186/s12891-021-04816-2. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
