

A digital mask to safeguard patient privacy
- PMID: 36109638
- PMCID: PMC9499857
- DOI: 10.1038/s41591-022-01966-1
A digital mask to safeguard patient privacy
Abstract
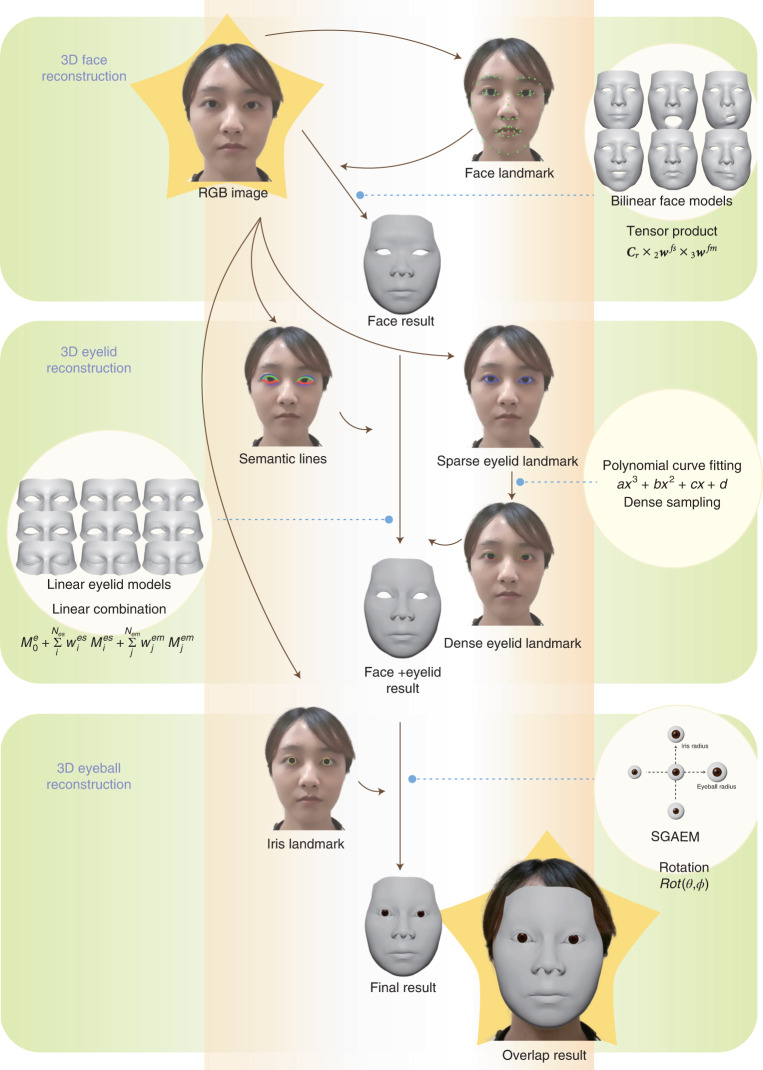
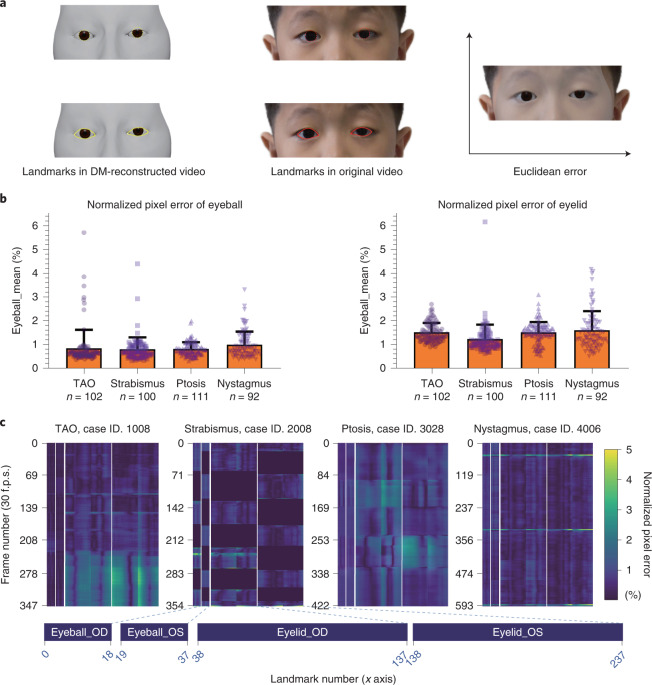
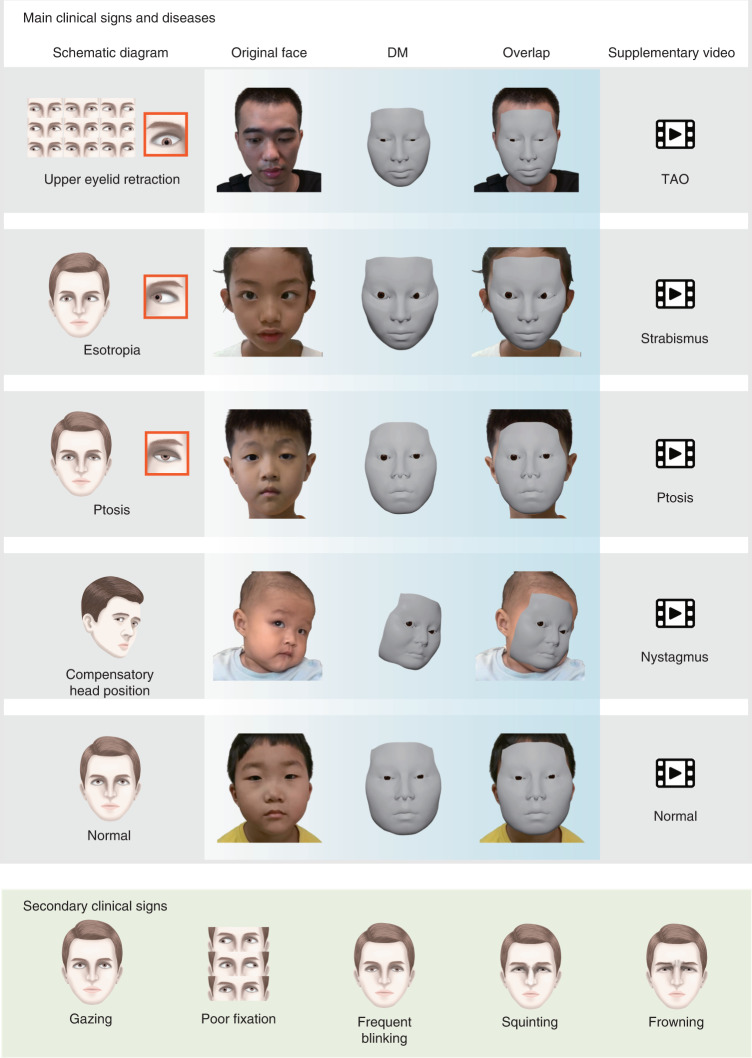
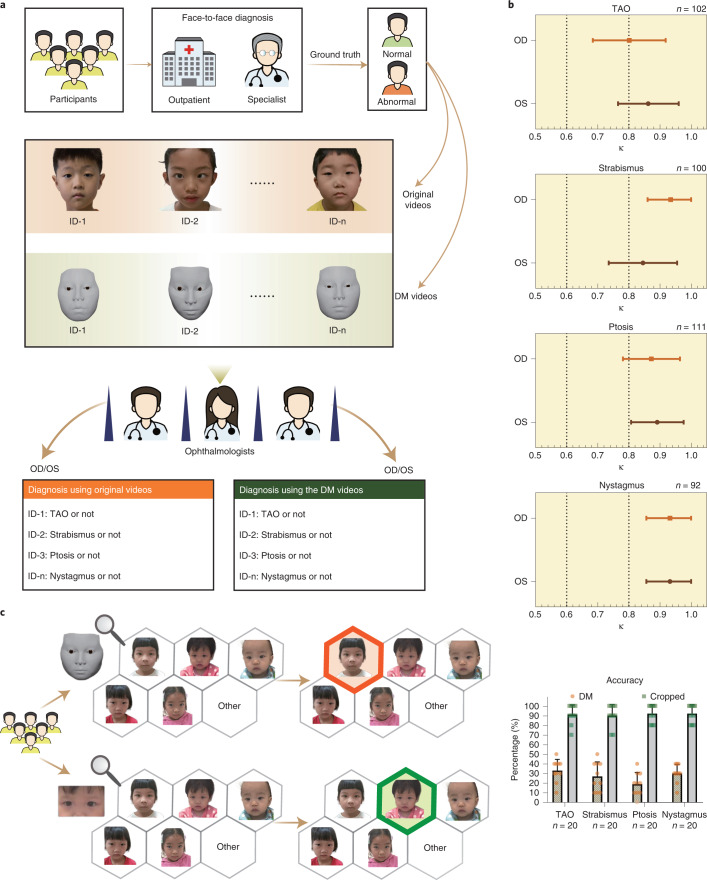
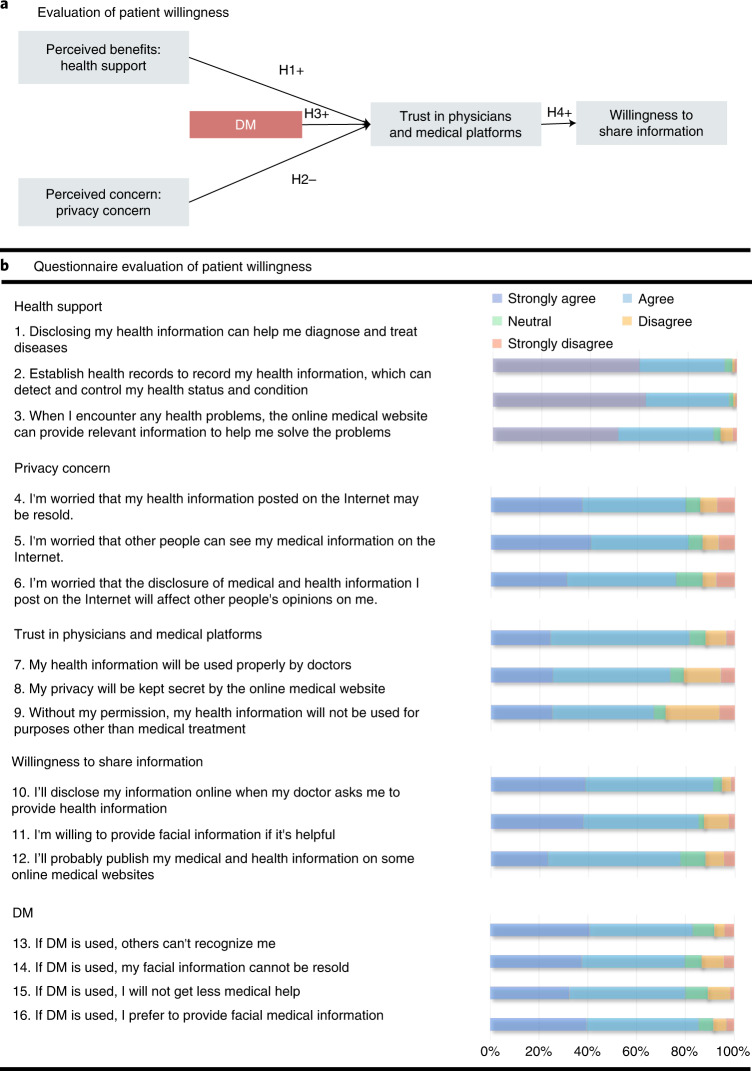
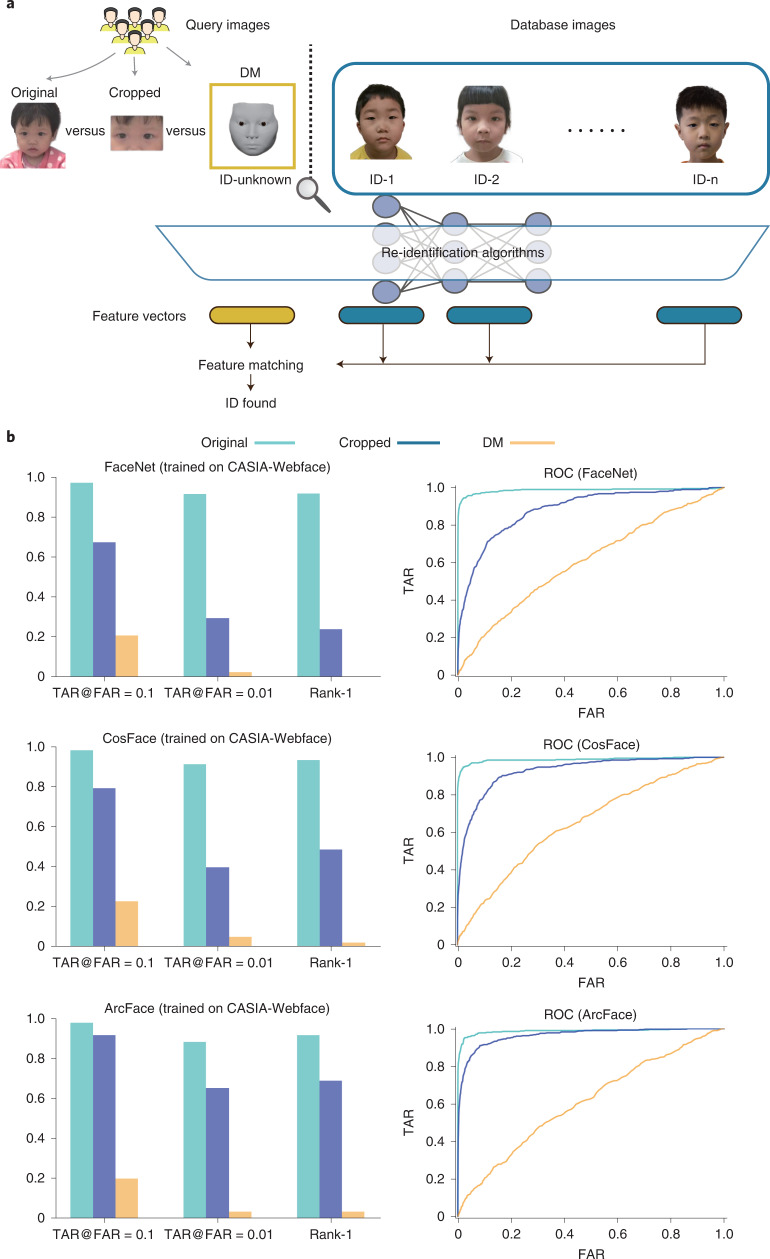
The storage of facial images in medical records poses privacy risks due to the sensitive nature of the personal biometric information that can be extracted from such images. To minimize these risks, we developed a new technology, called the digital mask (DM), which is based on three-dimensional reconstruction and deep-learning algorithms to irreversibly erase identifiable features, while retaining disease-relevant features needed for diagnosis. In a prospective clinical study to evaluate the technology for diagnosis of ocular conditions, we found very high diagnostic consistency between the use of original and reconstructed facial videos (κ ≥ 0.845 for strabismus, ptosis and nystagmus, and κ = 0.801 for thyroid-associated orbitopathy) and comparable diagnostic accuracy (P ≥ 0.131 for all ocular conditions tested) was observed. Identity removal validation using multiple-choice questions showed that compared to image cropping, the DM could much more effectively remove identity attributes from facial images. We further confirmed the ability of the DM to evade recognition systems using artificial intelligence-powered re-identification algorithms. Moreover, use of the DM increased the willingness of patients with ocular conditions to provide their facial images as health information during medical treatment. These results indicate the potential of the DM algorithm to protect the privacy of patients' facial images in an era of rapid adoption of digital health technologies.
© 2022. The Author(s).
Conflict of interest statement
Zhongshan Ophthalmic Center and Tsinghua University have filed for patent protection for H.L., F.X., Y.Y., R.W. and J.L. for work related to patient privacy protection method. All other authors declare no competing interests.
Figures
Comment in
-
Concerns about using a digital mask to safeguard patient privacy.Nat Med. 2023 Jul;29(7):1658-1659. doi: 10.1038/s41591-023-02439-9. Epub 2023 Jul 18. Nat Med. 2023. PMID: 37464037 Free PMC article. No abstract available.
-
Reply to: Concerns about using a digital mask to safeguard patient privacy.Nat Med. 2023 Jul;29(7):1660-1661. doi: 10.1038/s41591-023-02435-z. Epub 2023 Jul 18. Nat Med. 2023. PMID: 37464038 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
