

The association of Serratus Anterior Plane blocks with postoperative opioid use and analgesia following simple lumpectomy: a retrospective cohort analysis
- PMID: 36109719
- PMCID: PMC9476687
- DOI: 10.1186/s12871-022-01834-y
The association of Serratus Anterior Plane blocks with postoperative opioid use and analgesia following simple lumpectomy: a retrospective cohort analysis
Abstract
Background: The potential benefit of regional interventions for simple lumpectomy breast cancer surgeries has not been well investigated. Understanding which patients to not offer a regional intervention to can be just as important as knowing which would benefit. It is unclear whether fascial plane blocks, such as serratus anterior plane (SAP) block, should be routinely performed for less extensive breast surgeries. Therefore, our goal in this retrospective cohort study was to evaluate the association of integrating SAP blocks into a standard perioperative multimodal analgesia plan in patients undergoing simple lumpectomies (without node biopsies) with perioperative opioid consumption. As secondary outcomes, we also analyzed postoperative pain scores and post-anesthesia care unit (PACU) length of stay.
Methods: This was a single institution retrospective cohort study (surgical site infiltration only versus SAP block cohorts) assessing the association of SAP blocks to our outcomes of interest. In the adjusted analysis, we created matched cohorts using 1:1 (surgical site infiltration only: SAP block) propensity-score matching using nearest neighbor-matching without replacement. To compare the primary and secondary outcomes in the matched cohorts, we used the Wilcoxon signed rank test. A P-value of < 0.05 was considered statistically significant.
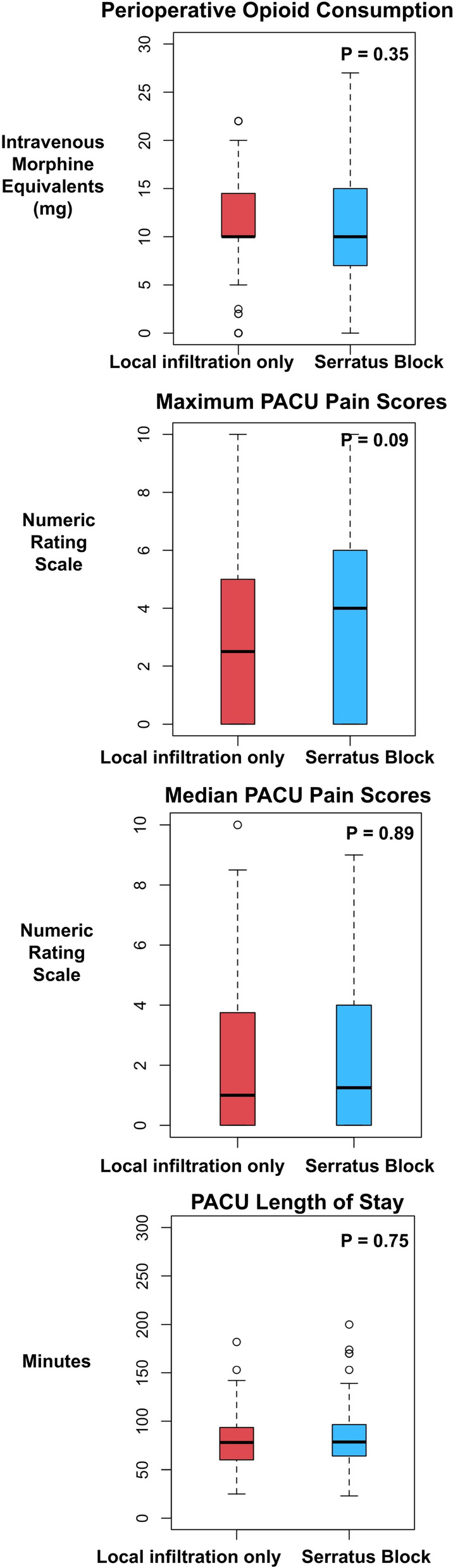
Results: There were 419 patients included in the analysis, in which 116 (27.7%) received a SAP block preoperatively in addition to our standard perioperative analgesia plan. In an unadjusted analysis, no differences were seen in perioperative opioid consumption, PACU pain scores, and PACU length of stay. Among the matched cohorts, the median [quartile] perioperative opioid consumption in the surgical site infiltration only versus SAP block cohorts were 10 mg [10, 13.25 mg] and 10 mg [7, 15 mg], respectively (P = 0.16). No differences were seen in the other outcomes.
Conclusions: In this study, we evaluated the impact of SAP blocks on patients undergoing simple lumpectomies, which are relatively less involved breast surgeries. We concluded that routine use of preoperative regional anesthesia is not beneficial for these specific patients. Future studies should focus on identifying patients that would directly benefit from regional interventions.
Keywords: Breast surgery; Enhanced recovery after surgery; Lumpectomy; Regional anesthesiology; Serratus anterior plane.
© 2022. The Author(s).
Conflict of interest statement
None.
Figures
Similar articles
-
Pectoralis I and Serratus Anterior Plane Block Analgesia for Bilateral Mastectomy: A Case Series.Pain Physician. 2024 Dec;27(10):E1117-E1122. Pain Physician. 2024. PMID: 39688831
-
Intraoperative Fascial Plane Blocks Facilitate Earlier Tracheal Extubation and Intensive Care Unit Discharge After Cardiac Surgery: A Retrospective Cohort Analysis.J Cardiothorac Vasc Anesth. 2023 Mar;37(3):437-444. doi: 10.1053/j.jvca.2022.11.021. Epub 2022 Nov 26. J Cardiothorac Vasc Anesth. 2023. PMID: 36566128
-
Pectoralis and Serratus Fascial Plane Blocks Each Provide Early Analgesic Benefits Following Ambulatory Breast Cancer Surgery: A Retrospective Propensity-Matched Cohort Study.Anesth Analg. 2017 Jul;125(1):294-302. doi: 10.1213/ANE.0000000000001975. Anesth Analg. 2017. PMID: 28328756
-
Benefits of Transversus Abdominis Plane Block on Postoperative Analgesia after Bariatric Surgery: A Systematic Review and Meta-Analysis.Pain Physician. 2021 Aug;24(5):345-358. Pain Physician. 2021. PMID: 34323436
-
Contribution of Multimodal Analgesia to Postoperative Pain Outcomes Immediately After Primary Anterior Cruciate Ligament Reconstruction: A Systematic Review and Meta-analysis of Level 1 Randomized Clinical Trials.Am J Sports Med. 2021 Sep;49(11):3132-3144. doi: 10.1177/0363546520980429. Epub 2021 Jan 7. Am J Sports Med. 2021. PMID: 33411564
References
-
- Wang L, Cohen JC, Devasenapathy N, Hong BY, Kheyson S, Lu D, et al. Prevalence and intensity of persistent post-surgical pain following breast cancer surgery: a systematic review and meta-analysis of observational studies. Br J Anaesth. 2020;125(3):346–357. doi: 10.1016/j.bja.2020.04.088. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
