

Robot-assisted Bladder Diverticulectomy Using a Transperitoneal Extravesical Approach
- PMID: 36110902
- PMCID: PMC9468349
- DOI: 10.1016/j.euros.2022.08.016
Robot-assisted Bladder Diverticulectomy Using a Transperitoneal Extravesical Approach
Abstract
Background: Acquired bladder diverticula (BD) are a possible complication of bladder outlet obstruction (BOO) due to benign prostate enlargement (BPE). Robot-assisted bladder diverticulectomy (RABD) has been proposed as an alternative to open removal; however, only a few small series have been published.
Objective: To describe our surgical technique for RABD and to assess perioperative results and functional outcomes at 6-mo follow-up.
Design setting and participants: A prospective single-centre, single-surgeon cohort of 16 consecutive men with posterior or posterolateral BD due to BOO/BPE undergoing RABD between May 2017 and December 2021 was analysed.
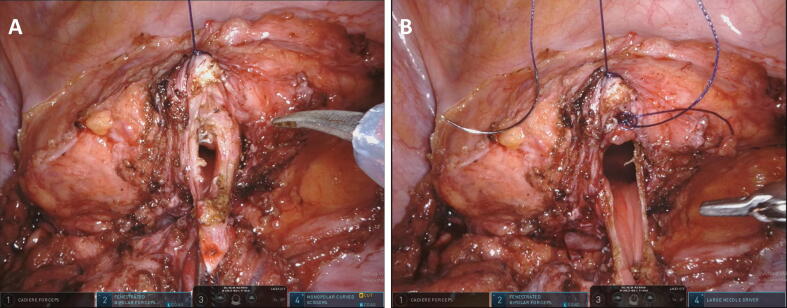
Surgical procedure: RABD was performed with a four-arm robotic system via a transperitoneal approach. BD were identified intraoperatively via bladder distension with saline solution through an indwelling catheter with or without concomitant illumination using flexible cystoscopy and fluorescence imaging. Extravesical BD dissection and removal were performed.
Outcome measurements and statistical analysis: Operating room time, estimated blood loss, intraoperative and postoperative complications, indwelling catheter time, and timing of associated procedures for BOO/BPE were assessed. The International Prostate Symptom Score (IPSS) and postvoid residual volume (PVR) were compared between baseline and 6 mo after surgery.
Results and limitations: Median age and maximum BD diameter were 68 yr (interquartile range [IQR] 54-74) and 69 mm (IQR 51-82), respectively. The median operative time was 126 min (IQR 92-167) and the median estimated blood loss was 20 ml (IQR 15-40). No intraoperative complications were recorded. The urethral catheter was removed on median postoperative day 5 (IQR 5-7). Two men experienced 90-d postoperative complications (persistent urinary infection requiring prolonged antimicrobial therapy). Bipolar transurethral resection of the prostate was performed 3 wk before RABD in seven men and concomitant to RABD in nine men. Median IPSS significantly decreased from 25 (IQR 21-30) to 5 (IQR 5-6), and median PVR from 195 ml (IQR 140-210 ml) to 30 (IQR 28-40) ml (both p < 0.001) at 6-mo follow-up in comparison to baseline. A limitation is the rather small cohort with no control group.
Conclusions: RABD is a safe and effective minimally invasive option for treatment of acquired BD in men with BOO/BPE. Validation of our results in larger series with longer follow-up is warranted.
Patient summary: We describe our surgical technique for robot-assisted removal of pouches in the bladder wall (called diverticula) in men with bladder outlet obstruction caused by benign prostate enlargement, and report functional results at 6 months after the operation. This minimally invasive technique was found to be safe and effective.
Keywords: Benign prostate enlargement; Benign prostate hyperplasia; Bladder; Bladder diverticulectomy; Bladder outlet obstruction; Diverticulum; Lower urinary tract symptoms; Robot-assisted surgery.
© 2022 The Author(s).
Figures


References
-
- Moreno Sierra J., Galante-Romo I., Ortiz-Oshiro E., Castillon-Vela I.T., Fernandez-Perez C., Silmi-Moyano A. Bladder diverticulum robotic surgery: systematic review of case reports. Urol Int. 2010;85:381–385. - PubMed
-
- Walker N.F., Gan C., Olsburgh J., Khan M.S. Diagnosis and management of intradiverticular bladder tumours. Nat Rev Urol. 2014;11:383–390. - PubMed
-
- Pacella M., Testino N., Mantica G., Valcalda M., Malinaric R., Terrone C. Transurethral endoscopic approach for large bladder diverticula: evaluation of a large series. Arch Ital Urol Androl. 2019;91:174–176. - PubMed
-
- Parra R.O., Jones J.P., Andrus C.H., Hagood P.G. Laparoscopic diverticulectomy: preliminary report of a new approach for the treatment of bladder diverticulum. J Urol. 1992;148:869–871. - PubMed
-
- Berger A.D., Stifelman M.D. Robotic bladder diverticulectomy: initial experience. J Urol. 2006;175(Suppl 4):V501.
LinkOut - more resources
Full Text Sources
Research Materials
