

Surgical Results and Complications for Open, Laparoscopic, and Robot-assisted Radical Prostatectomy: A Reverse Systematic Review
- PMID: 36110904
- PMCID: PMC9468352
- DOI: 10.1016/j.euros.2022.08.015
Surgical Results and Complications for Open, Laparoscopic, and Robot-assisted Radical Prostatectomy: A Reverse Systematic Review
Abstract
Context: The advantages of minimally invasive surgery for radical prostatectomy (RP) have been demonstrated in a number of systematic reviews (SRs). However, the rigorous study selection process for SR means that a lot of information can be excluded, leading to a very specific clinical scenario that is often unrepresentative of real life. Our new reverse SR methodology generates a heterogeneous population database that covers a wide range of clinical scenarios.
Objective: To compare perioperative surgical results and complications for open retropubic RP (RRP), laparoscopic RP (LRP), and robot-assisted RP (RARP) in a reverse SR.
Evidence acquisition: Eight databases were searched for SRs on RRP, LRP, or RARP between 2000 and 2020 (80 SRs). All references used in these SRs were captured for analysis (1724 articles). Perioperative outcomes and complications were compared among the RRP, LRP, and RARP approaches.
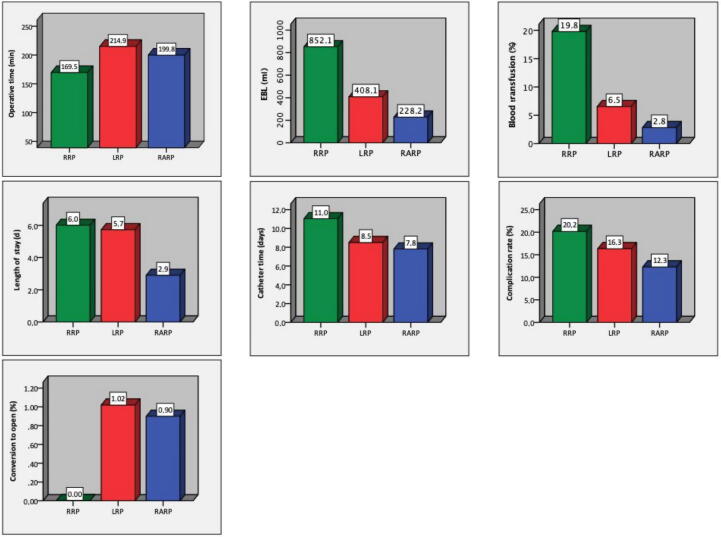
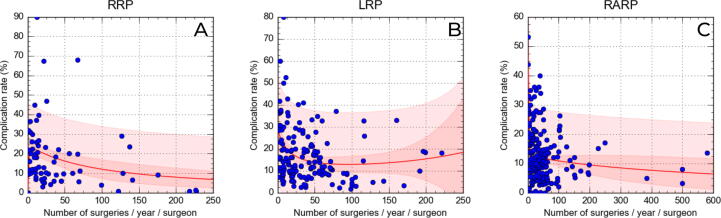
Evidence synthesis: We identified 559 (32.4%) reports on RRP, 413 (23.9%) on LRP, and 752 (43.7%) on RARP, involving 1 353 485 patients overall. RARP showed a significantly higher annual volume of surgery per surgeon (AVSS) in comparison to RRP and LRP (mean 64.29, 43.26, and 41.47, respectively), a higher percentage of low-risk patients (prostate-specific antigen <10 ng/ml, Gleason <7, stage <cT2), and a lower rate of lymphadenectomy, culminating in a lower complication rate (12.3% for RARP, 16.3% for LRP, 20.2% for RRP). Among all outcomes, only AVSS was significantly correlated with complication rates. An AVSS of 30, 95 and 95 surgeries/yr was required for RARP, LRP, and RRP, respectively, to obtain a complication rate of 12.3% (average for RARP). RARP showed better performance for all perioperative variables studied except for operative time (operative time: 199.8 vs 214.9 vs 169.5 min; estimated blood loss: 228.2 vs 408.0 vs 852.1 ml; blood transfusion rate: 2.8% vs 6.5% vs 19.8%; length of stay: 2.9 vs 5.7 vs 6.1 d; catheter time: 7.8 vs 8.5 vs 11.0 d for RARP vs LRP vs RRP).
Conclusions: Our reverse SR involved a wide real-life representative sample and reference values established in the literature and revealed that minimally invasive surgery had the best perioperative and complication results, especially RARP, which was associated with less complex cases, higher annual surgeon volume, and greater performance.
Patient summary: We used a wide sample representative of real-life surgical practice and reference values established in the literature for three techniques for removal of the prostate to guide patients and physicians in deciding the best surgical treatment for prostate cancer according to availability.
Keywords: Complications; Laparoscopic surgery; Methodology; Open surgery; Radical prostatectomy; Reverse systematic review; Robot-assisted surgery.
© 2022 The Authors.
Figures

References
-
- Sanda M.G., Cadeddu J.A., Kirkby E., et al. Clinically localized prostate cancer: AUA/ASTRO/SUO guideline. Part I: risk stratification, shared decision making, and care options. J Urol. 2018;199:683–690. - PubMed
-
- Mottet N., Cornford P., van den Bergh R.C.N., et al. European Association of Urology; Arnhem, The Netherlands: 2022. EAU guidelines: prostate cancer.
-
- Moretti T.B.C., Magna L.A., Reis L.O. Development and application of reverse systematic review on laparoscopic radical prostatectomy. Urol Oncol. 2019;37:647–658. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
