

Chondroitin sulfate proteoglycan 4 expression in chondrosarcoma: A potential target for antibody-based immunotherapy
- PMID: 36110930
- PMCID: PMC9468862
- DOI: 10.3389/fonc.2022.939166
Chondroitin sulfate proteoglycan 4 expression in chondrosarcoma: A potential target for antibody-based immunotherapy
Abstract
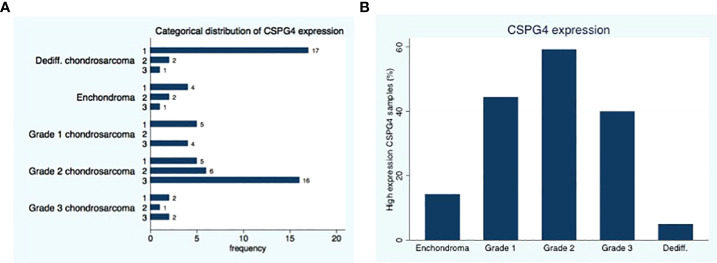
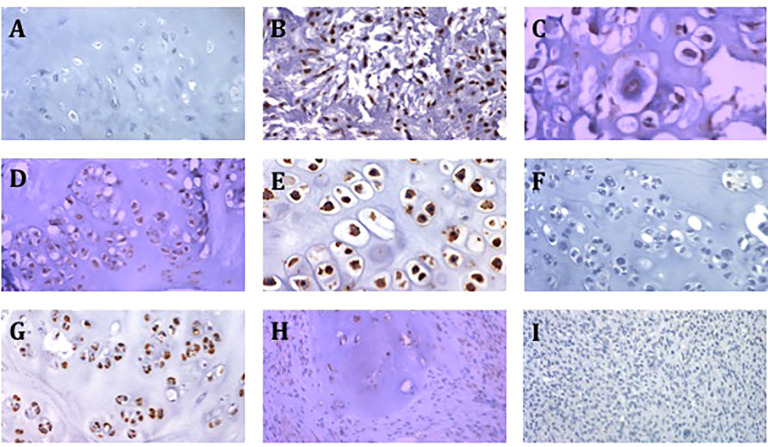
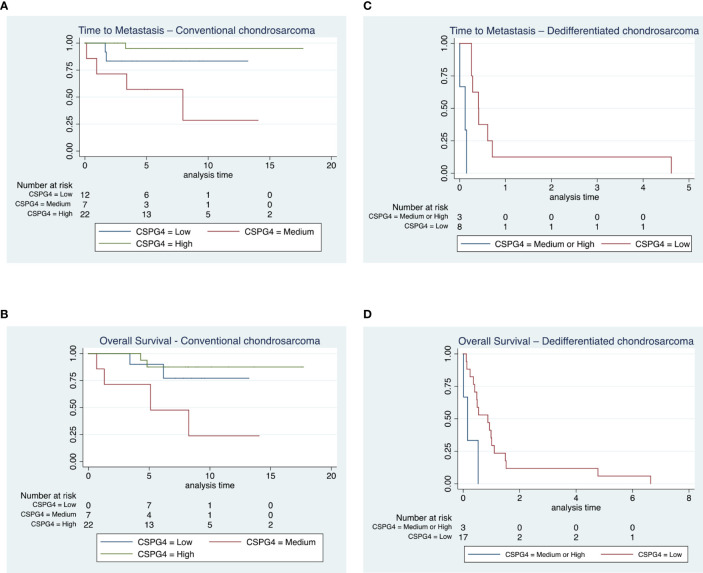
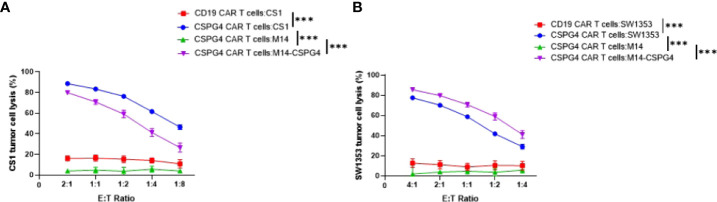
Chondrosarcoma is a common primary bone malignancy whose phenotype increases with its histologic grade. They are relatively resistant to chemotherapy and radiation therapy limiting curative options for disseminated disease. Chondroitin sulfate proteoglycan 4 (CSPG4) is a cell surface proteoglycan that is highly expressed across various human cancers, including chondrosarcoma, and has restricted distribution in healthy tissues, making it an attractive target for the antibody-based therapy. CSPG4 specific chimeric antigen receptor (CAR) T cell therapies have been shown to be effective in treating other cancers such as melanoma and triple negative breast cancer. The goal of this study was to assess the prevalence of CSPG4 in human chondrosarcoma and to assess the efficacy of CSPG4 specific CAR T cells in lysing chondrosarcoma cells in vitro. Using immunohistochemistry (IHC), we stained a tissue microarray containing primary conventional and dedifferentiated chondrosarcoma from 76 patients with CSPG4 specific monoclonal antibodies (mAbs). In addition, we incubated 2 chondrosarcoma cell lines with CSPG4-targeting CAR T cells and subsequently evaluated cell survival. Our results showed medium to high expression of CSPG4 in 29 of 41 (71%) conventional chondrosarcoma tumors and in 3 of 20 (15%) dedifferentiated chondrosarcoma tumors. CSPG4 expression showed a positive association with time to metastasis and survival in both subtypes. CSPG4 CAR T treated cell lines showed a lysis of respectively >80% and 70% demonstrating CSPG4-targeted CAR T cells effective in killing CSPG4-positive chondrosarcoma tumors.
Keywords: CAR T; CSPG4; chondrosarcoma; dedifferentiated chondrosarcoma; immunotherapy.
Copyright © 2022 Nota, Osei-Hwedieh, Drum, Wang, Sabbatino, Ferrone and Schwab.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Limaiem F, Davis DD, Sticco KL. Chondrosarcoma. StatPearls. Treasure Island (FL: StatPearls Publishing Copyright © 2022, StatPearls Publishing LLC. (2022).
-
- Shariat Torbaghan S, Ashouri M, Jalayer Naderi N, Baherini N. Histopathologic differentiation between enchondroma and well-differentiated chondrosarcoma: Evaluating the efficacy of diagnostic histologic structures. J Dental Res Dental Clin Dental Prospects (2011) 5:98–101. doi: 10.5681/joddd.2011.022 - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources