

A comprehensive framework of the right posterior section for tailored anatomical liver resection based on three-dimensional simulation system
- PMID: 36111052
- PMCID: PMC9469113
- DOI: 10.21037/atm-22-1105
A comprehensive framework of the right posterior section for tailored anatomical liver resection based on three-dimensional simulation system
Abstract
Background: The anatomical right posterior sectionectomy (ARPS) is a technically challenging procedure. We aimed to develop and validate a novel framework of the right posterior section for a safe and tailored anatomical liver resection (ALR) based on a three-dimensional (3D) simulation system.
Methods: 3D hepatectomy simulations of healthy participants who underwent contrast-enhanced computed tomography of the upper abdomen were retrospectively reviewed to develop the framework according to the relationship between the simulated plane determined by the right posterior portal pedicle (RPP) and the course of the right hepatic vein (RHV) trunk. The framework was validated in the practice of ARPS for hepatocellular carcinoma (HCC) prospectively.
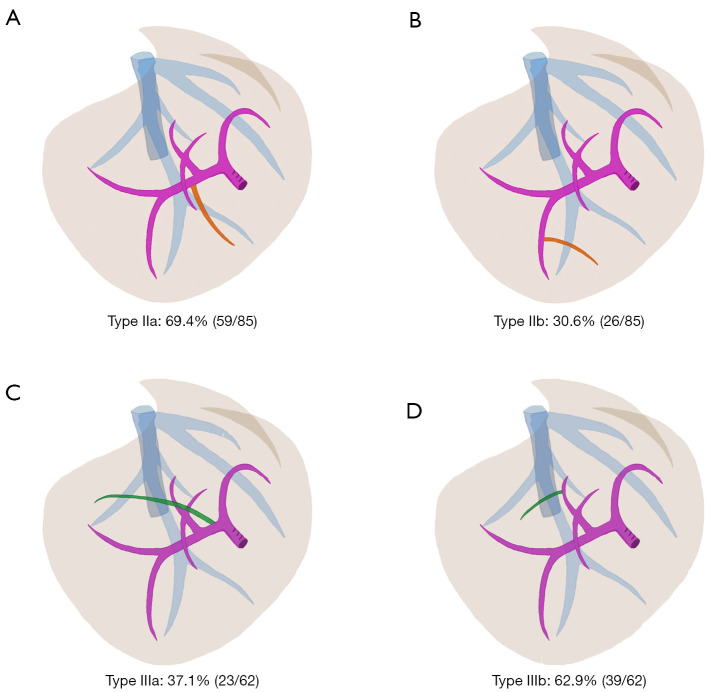
Results: Scans from 336 eligible participants were assessed. The framework was summarized into four types: normal, caudal-redundant, cranial-deficient, and combined types, accounting for 43.4% (146/336), 25.3% (85/336), 18.5% (62/336), and 12.8% (43/336) respectively. The caudal-redundant type was associated with the variable portal branches of the RPP or segment 6 branch across the ventral side of RHV. The mean aberrant volume proportion in type IIa was significantly greater than that in type IIb (P<0.001), which were 7.0%±3.5% and 4.4%±1.8% respectively. The cranial-deficient type was associated with the aberrant segment 7 portal pedicle originating from the right portal trunk or the dorsal portal branch of segment 8 crossing over to the RHV. The median aberrant volume proportion in type IIIa was significantly greater than that in type IIIb (P<0.001), which were 10.9% (8.5-13.3%) and 4.0% (3.0-6.1%), respectively. The combined type represented a combination of the caudal-redundant type and the cranial-deficient type. The framework provided instructions on tailored ARPS in 6 patients with HCC by maximizing lesion removal and functional liver remnant with favorable perioperative outcomes.
Conclusions: Precise preoperative planning with an individualized surgical approach based on our framework allows safe anatomical liver resections for cases with lesions in the right posterior section.
Keywords: Anatomical liver resection (ALR); computed tomography; outcomes; right posterior section; three-dimensional visualization.
2022 Annals of Translational Medicine. All rights reserved.
Conflict of interest statement
Conflicts of Interest: All authors have completed the ICMJE uniform disclosure form (available at https://atm.amegroups.com/article/view/10.21037/atm-22-1105/coif). The authors have no conflicts of interest to declare.
Figures






Comment in
-
Too much or insufficient information for anatomical right posterior sectionectomy?Ann Transl Med. 2022 Dec;10(24):1301. doi: 10.21037/atm-22-5587. Ann Transl Med. 2022. PMID: 36660700 Free PMC article. No abstract available.
-
Liver anatomy is king, three-dimensional reconstruction is queen, liver resections are princesses and princes.Ann Transl Med. 2022 Dec;10(24):1296. doi: 10.21037/atm-22-5247. Ann Transl Med. 2022. PMID: 36660713 Free PMC article. No abstract available.
References
LinkOut - more resources
Full Text Sources
Miscellaneous