

Incidence and impact of atrial fibrillation in heart failure patients: real-world data in a large community
- PMID: 36111519
- PMCID: PMC9773729
- DOI: 10.1002/ehf2.14124
Incidence and impact of atrial fibrillation in heart failure patients: real-world data in a large community
Abstract
Aims: The objective of the present study is to assess the bidirectional association between heart failure (HF) and atrial fibrillation (AF) using real-world data.
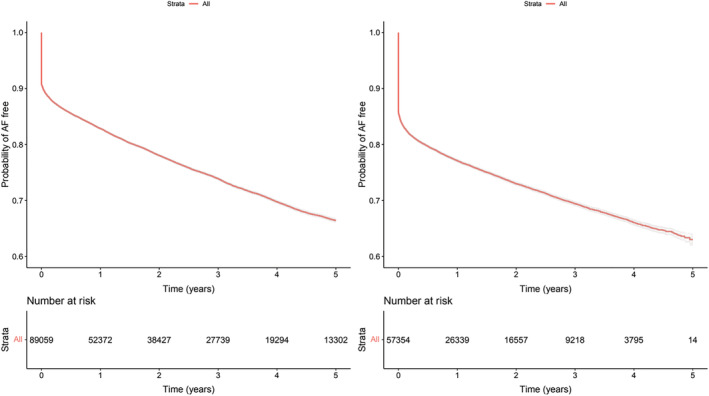
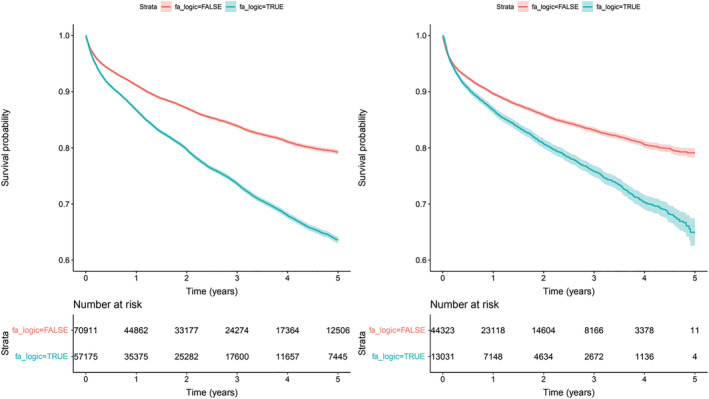
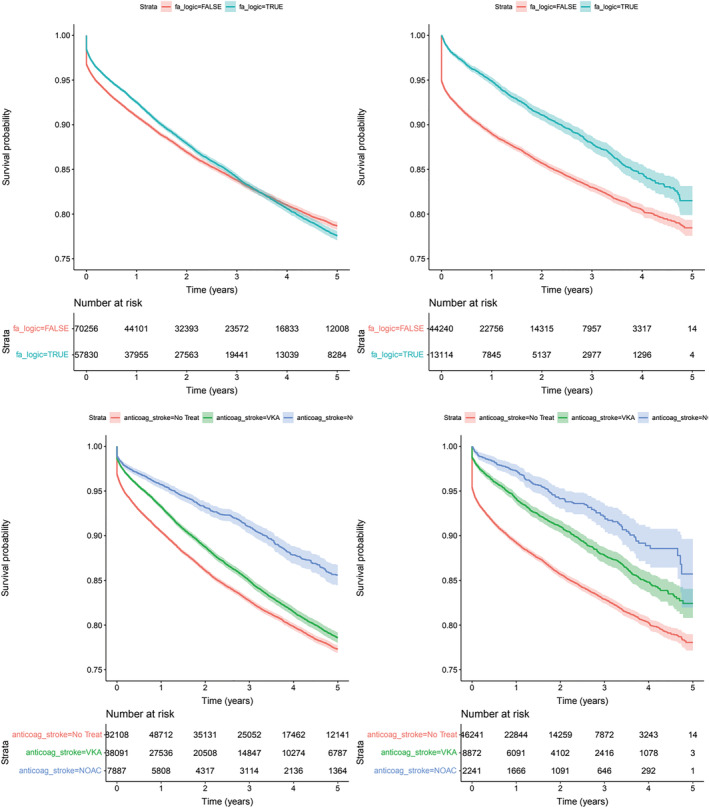
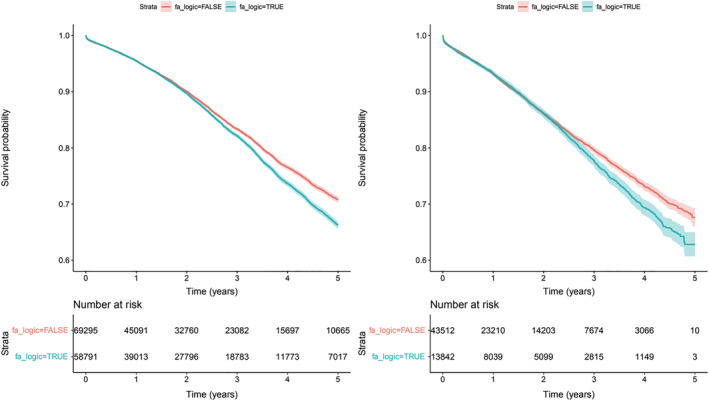
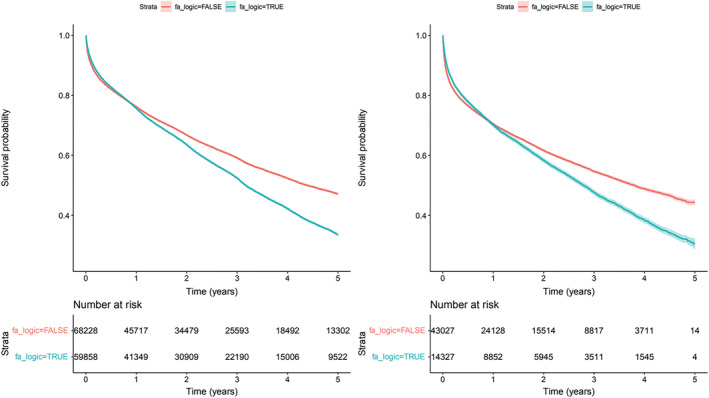
Methods and results: From an electronic health recording with a population of 3 799 885 adult subjects, those with prevalent or incident HF were selected and followed throughout a study period of 5 years. Prevalence and incidence of AF, and their impact in the risk for acute HF hospitalization, worsening renal function, ischaemic and haemorrhagic stroke, and all-cause mortality were identified. We analysed all incident and prevalent patients with HF and AF, 128 086 patients (S1), and subsequently analysed a subset of patients with incident HF and AF, 57 354 patients (S2). We analysed all incident and prevalent patients with HF and AF, 128 086 patients (S1), and subsequently a subset of patients with incident HF and AF, 57 354 patients (S2). The prevalence of AF was 59 906 (46.7%) of the HF patients, while incidence in the S2 was 231/1000 patients/year. In both cohorts, S1 and S2, AF significantly increases the risk of acute heart failure hospitalization [incidence 79.1/1000 and 97.5/1000 patients/year; HR 1.53 (1.48-1.59 95% CI) and HR 1.32 (1.24-1.41 95% CI), respectively], risk of decreased renal function (eGFR reduced by >20%) [66.2/1000 and 94.0/1000 patients/year; HR 1.13 (1.09-1.18 95% CI) and HR 1.22 (1.14-1.31 95% CI), respectively] and all-cause mortality [203/1000 and 294/1000 patients/year; HR 1.62 (1.58-1.65 95% CI) and HR 1.65 (1.59-1.70 95% CI), respectively]. The number of episodes of hospitalization for acute heart failure was also significantly higher in the AF patients (27 623 vs. 10 036, P < 0.001). However, the risk for ischaemic stroke was reduced in the AF subjects [HR 0.66 (0.63-0.74 95% CI)], probably due to the anticoagulant treatment.
Conclusions: AF is associated with an increment in the risk of episodes of acute heart failure as well as decline of renal function and increment of all-cause mortality.
Keywords: All-cause mortality; Atrial fibrillation; Heart failure; Hospitalization; Renal function; Stroke.
© 2022 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of European Society of Cardiology.
Conflict of interest statement
None declared.
Figures
References
-
- Michaud GF, Stevenson WG. Atrial Fibrillation. N Engl J Med. 2021; 384: 353–361. - PubMed
-
- John RM, Michaud GF, Stevenson WG. Atrial fibrillation hospitalization, mortality, and therapy. Eur Heart J. 2018; 39: 3958–3960. - PubMed
-
- Nedkoff L, Kelty EA, Hung J, Thompson SC, Katzenellenbogen JM. Differences in stroke risk and cardiovascular mortality for aboriginal and other Australian patients with atrial fibrillation. Med J Aust. 2020; 212: 215–221. - PubMed
-
- Pandey A, Kim S, Moore C, Thomas L, Gersh B, Allen LA, Kowey PR, Mahaffey KW, Hylek E, Peterson ED, Piccini JP, Fonarow GC. ORBIT‐AF investigators and patients. Predictors and prognostic implications of incident heart failure in patients with prevalent atrial fibrillation. JACC Heart Fail. 2017; 5: 44–52. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
