

Residential proximity to a fertility clinic is independently associated with likelihood of women having ART and IUI treatment
- PMID: 36112009
- PMCID: PMC9627258
- DOI: 10.1093/humrep/deac205
Residential proximity to a fertility clinic is independently associated with likelihood of women having ART and IUI treatment
Abstract
Study question: Is geographic proximity to a fertility clinic associated with the likelihood of women of reproductive age undertaking different forms of medically assisted fertility treatment?
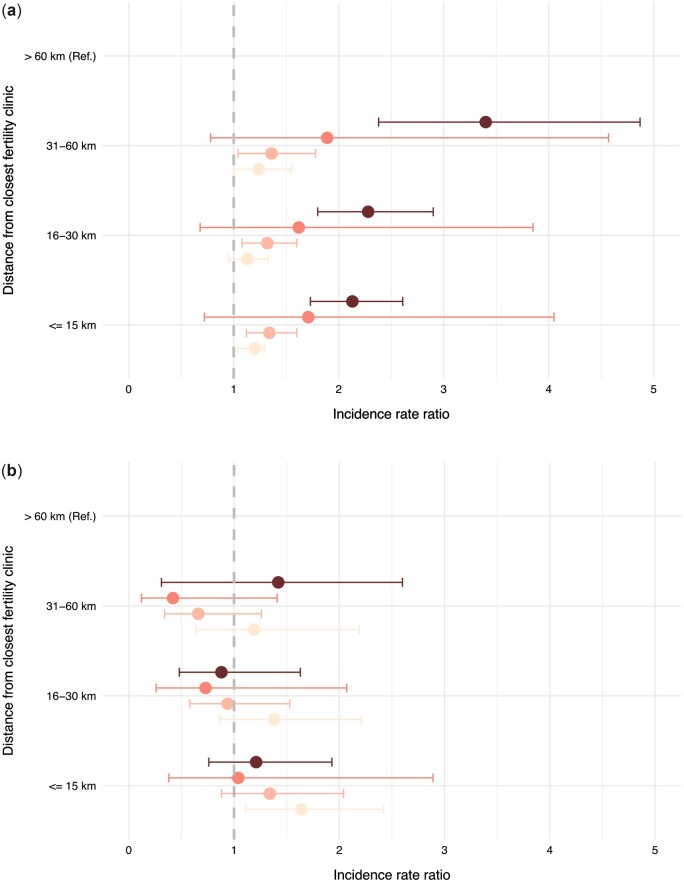
Summary answer: After adjusting for socioeconomic status (SES) and other confounders including a proxy for the need for infertility treatment, women who lived within 15 km of a fertility clinic were 21% more likely to undergo ART treatment and 68% more likely to undergo IUI treatment than those who lived further than 60 km away.
What is known already: In most countries, patients living outside of metropolitan areas are more likely to be more socio-economically disadvantaged and to have less equitable access to healthcare. However, how a woman's residential proximity to fertility clinics predicts utilization of high-cost/high-technology treatment (ART) and low-cost/low-technology treatment (IUI) is limited, and whether socio-economic disadvantage explains much of the hypothesized lower utilization is unknown. Australia's universal insurance scheme provides supportive reimbursement for almost all ART and IUI treatment regardless of age or number of cycles, providing a unique setting to investigate disparities in access to infertility treatment.
Study design, size, duration: National population-based observation study of ART and IUI treatment utilization by women across socio-economic gradients and Australian residential locations between August 2015 and December 2017.
Participants/materials, setting, methods: Universal insurance claims information on female patients who underwent ART or IUI were provided by Services Australia, comprising 67 670 female patients who accessed 162 795 ART treatments, and 10 211 female patients who accessed 19 615 IUI treatments over a 29-month period. Incidence rates by SES and proximity to fertility clinics were calculated to describe the number of women undergoing at least one ART or IUI treatment cycle per 1000 women of reproductive age (25-44). Treatment frequencies were calculated to describe the average number of ART or IUI treatment cycles per woman of reproductive age who had undergone at least one ART or IUI treatment during the study period. Poisson regression analyses were used to estimate the independent effect on accessibility to infertility treatment by geographic proximity (based on small area locations) to the closest fertility clinic after adjusting for SES, childbearing delay, remoteness area, and marital status.
Main results and the role of chance: On average, 19.1 women per 1000 women of reproductive age underwent at least one fresh or frozen ART cycle, with an average 2.3 ART cycles each, while 3.0 women per 1000 women of reproductive age received at least one IUI cycle, with an average of 1.6 IUI cycles each. After adjusting for SES and other confounders including a proxy for the need for infertility treatment, women who lived within 15 km of a fertility clinic were 21% more likely to undergo ART treatment and 68% more likely to undergo IUI than those who lived over 60 km away. Regardless of geographic location, there was a steady and independent gradient in access to ART treatment based on increasing SES, with women residing in the most advantaged residential quartile having a 37% higher rate of receiving ART treatment compared to those in the most disadvantaged quartile. The negative effect of social disadvantage on ART use became more pronounced as distance from a fertility clinic grew, indicating that the barriers to access to ART care caused by distance were further compounded by the level of socioeconomic advantage of the women's residential location. In contrast, socioeconomic status did not modify the likelihood of using IUI over and above the distance from a fertility clinic. In relation to IUI treatment, differences in utilization by SES disappeared after adjusting for geographic proximity to a fertility clinic, childbearing delay, remoteness area, and marital status.
Limitations, reasons for caution: Information is aggregated by small geographic areas and it therefore may not reflect individual characteristics. Australia provides partial but comparably supportive reimbursement for both ART and IUI through its universal healthcare system and thus the results may not be fully generalizable to other settings.
Wider implications of the findings: Residential proximity to a fertility clinic is a persistent barrier to accessing ART and IUI treatment, regardless of SES, even in countries characterized by supportive public funding, such as Australia. SES is less of a barrier to accessing IUI than ART, presumably driven by the lower cost and fewer clinic visits required with IUI treatment. Safe and effective fertility treatment should be available to all women regardless of where they live.
Study funding/competing interest(s): This work was supported by the Australian National University Research scholarship and by the Higher Degree Research Fee Merit Scholarship. The authors have no conflict of interest.
Trial registration number: N/A.
Keywords: Australia; assisted reproductive technology; geographic accessibility; intrauterine insemination; medically assisted fertility treatments; social inequalities; utilization.
© The Author(s) 2022. Published by Oxford University Press on behalf of European Society of Human Reproduction and Embryology.
Figures
References
-
- AIHW. Rural & Remote Health. 2019. https://www.aihw.gov.au/reports/rural-remote-australians/rural-remote-he... (1 May 2022, date last accessed).
-
- Allan S, Balaban B, Banker M, Buster J, Horton M, Miller K, Mocanu E, Ory S, Pai H, can der Poel S. et al. International Federation of Fertility Societies’ Surveillance (IFFS) 2019: global trends in reproductive policy and practice, 8th Edition. Glob Reprod Health 2019;4:e29.
-
- Australian Bureau of Statistics. Australian Statistical Geography Standard (AGSC): Volume 1—Main Structure and Greater Capital City Statistical Areas, July 2016. 2016. www.abs.gov.au (15 August 2021, date last accessed).
-
- Australian Bureau of Statistics. Census of Population and Housing: Socio-Economic Indexes for Areas (SEIFAs), Australia, 2016. 2018a. www.abs.gov.au (15 August 2021, date last accessed).
-
- Australian Bureau of Statistics. The Australian Statistical Geography Standard (ASGS) Remoteness Structure (ASGC). 2018b. www.abs.gov.au (15 August 2021, date last accessed).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
