

Cardiac arrest and complications during non-invasive ventilation: a systematic review and meta-analysis with meta-regression
- PMID: 36112157
- PMCID: PMC9483519
- DOI: 10.1007/s00134-022-06821-y
Cardiac arrest and complications during non-invasive ventilation: a systematic review and meta-analysis with meta-regression
Abstract
Purpose: The aim of this study was to perform a systematic review and meta-analysis to investigate the incidence rate of cardiac arrest and severe complications occurring under non-invasive ventilation (NIV).
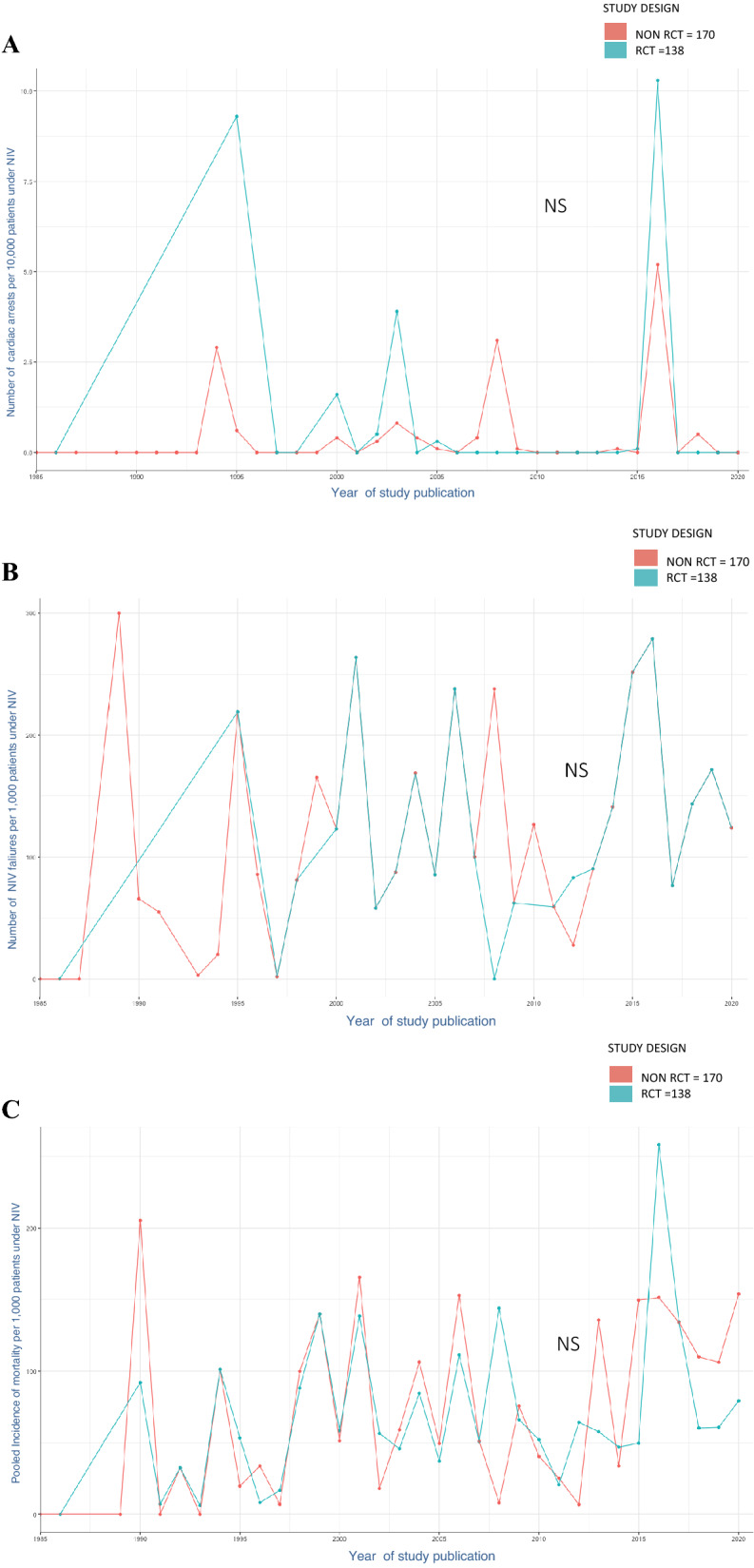
Methods: We performed a systematic review and meta-analysis of studies between 1981 and 2020 that enrolled adults in whom NIV was used to treat acute respiratory failure (ARF). We generated the pooled incidence and confidence interval (95% CI) of NIV-related cardiac arrest per patient (primary outcome) and performed a meta-regression to assess the association with study characteristics. We also generated the pooled incidences of NIV failure and hospital mortality.
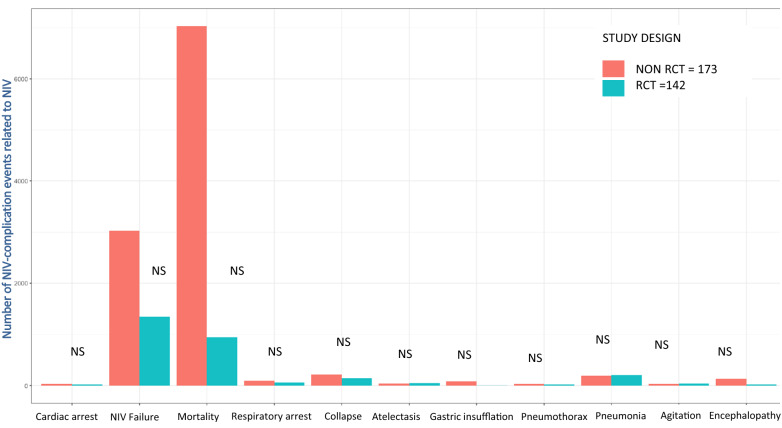
Results: Three hundred and eight studies included a total of 7,601,148 participants with 36,326 patients under NIV (8187 in 138 randomized controlled trials, 9783 in 99 prospective observational studies, and 18,356 in 71 retrospective studies). Only 19 (6%) of the analyzed studies reported the rate of NIV-related cardiac arrest. Forty-nine cardiac arrests were reported. The pooled incidence was 0.01% (95% CI 0.00-0.02, I2 = 0% (0-15)). NIV failure was reported in 4371 patients, with a pooled incidence of 11.1% (95% CI 9.0-13.3). After meta-regression, NIV failure and the study period (before 2010) were significantly associated with NIV-related cardiac arrest. The hospital mortality pooled incidence was 6.0% (95% CI 4.4-7.9).
Conclusion: Cardiac arrest related to NIV occurred in one per 10,000 patients under NIV for ARF treatment. NIV-related cardiac arrest was associated with NIV failure.
Keywords: Cardiac arrest; Complications; ICU; Meta-analysis; Non-invasive ventilation.
© 2022. Springer-Verlag GmbH Germany, part of Springer Nature.
Conflict of interest statement
SJ reports receiving consulting fees from Drager, Medtronic, Fresenius, Baxter, Mindray and Fisher & Paykel. ADJ reports receiving consulting fees from Drager, Medtronic and Fisher & Paykel. EA has received fees from Gilead Sciences, Alexion, Astellas, MSD and Drager. No potential conflicts of interest relevant to this article were reported for the other authors.
Figures


References
-
- Jaber S, Lescot T, Futier E, Paugam-Burtz C, Seguin P, Ferrandiere M, Lasocki S, Mimoz O, Hengy B, Sannini A, Pottecher J, Abback PS, Riu B, Belafia F, Constantin JM, Masseret E, Beaussier M, Verzilli D, De Jong A, Chanques G, Brochard L, Molinari N. Effect of noninvasive ventilation on tracheal reintubation among patients with hypoxemic respiratory failure following abdominal surgery: a randomized clinical trial. JAMA. 2016;315:1345–1353. doi: 10.1001/jama.2016.2706. - DOI - PubMed
-
- Demoule A, Chevret S, Carlucci A, Kouatchet A, Jaber S, Meziani F, Schmidt M, Schnell D, Clergue C, Aboab J, Rabbat A, Eon B, Guerin C, Georges H, Zuber B, Dellamonica J, Das V, Cousson J, Perez D, Brochard L, Azoulay E. Changing use of noninvasive ventilation in critically ill patients: trends over 15 years in francophone countries. Intensive Care Med. 2016;42:82–92. doi: 10.1007/s00134-015-4087-4. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
