

Treatment of Cryptococcal Meningitis: How Have We Got Here and Where are We Going?
- PMID: 36112342
- PMCID: PMC9483520
- DOI: 10.1007/s40265-022-01757-5
Treatment of Cryptococcal Meningitis: How Have We Got Here and Where are We Going?
Abstract
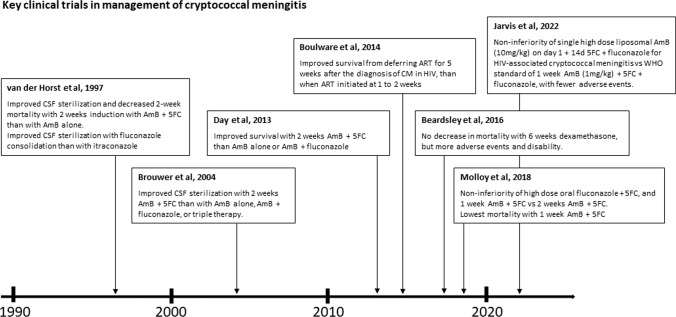
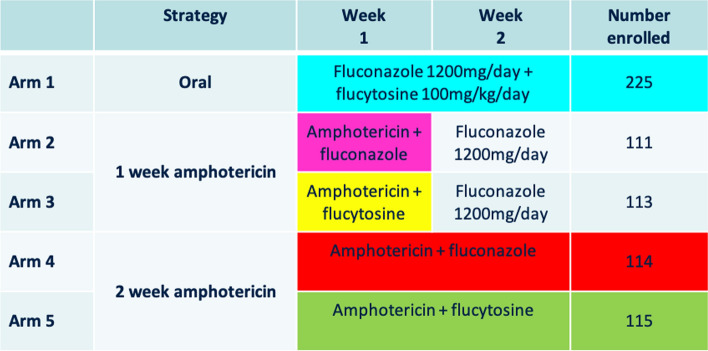
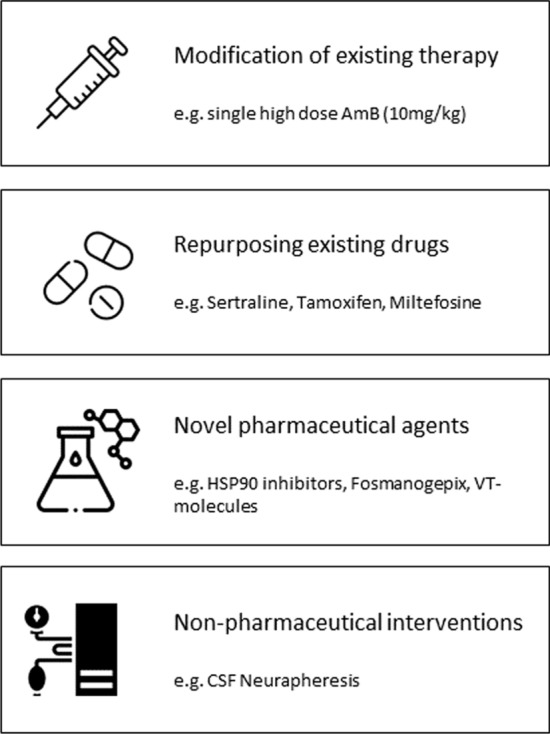
Cryptococcal meningitis is a devastating brain infection cause by encapsulated yeasts of the Cryptococcus genus. Exposure, through inhalation, is likely universal by adulthood, but symptomatic infection only occurs in a minority, in most cases, months or years after exposure. Disease has been described in almost all tissues, but it is the organism's tropism for the central nervous system that results in the most devastating illness. While invasive disease can occur in the immunocompetent, the greatest burden by far is in immunocompromised individuals, particularly people living with human immunodeficiency virus (HIV), organ transplant recipients and those on glucocorticoid therapy or other immunosuppressive drugs. Clinical presentation is variable, but diagnosis is usually straightforward, with cerebrospinal fluid microscopy, culture, and antigen testing proving significantly more sensitive than diagnostic tests for other brain infections. Although disease incidence has reduced since the advent of effective HIV therapy, mortality when disease occurs remains extremely high, and has changed little in recent decades. This Therapy in Practice review is an update of a talk first given by JND at the European Congress on Clinical Microbiology and Infectious Diseases in 2019 in the Netherlands. The review contextualizes the most recently published World Health Organization (WHO) guidelines for the treatment of HIV-associated cryptococcal meningitis in terms of the data from large, randomized, controlled trials published between 1997 and 2022. We discuss the rationale for induction and maintenance therapy and the efficacy and undesirable effects of the current therapeutic armamentarium of amphotericin, flucytosine and fluconazole. We address recent research into repurposed drugs such as sertraline and tamoxifen, and potential future treatment options, including the novel antifungals fosmanogepix, efungumab and oteseconazole, and non-pharmaceutical solutions such as neurapheresis cerebrospinal fluid filtration.
© 2022. The Author(s).
Conflict of interest statement
Drs. Day, Flower and Thuy declare that they have no conflicts of interest.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
