

Changes in Emergency Department Visits for Cannabis Hyperemesis Syndrome Following Recreational Cannabis Legalization and Subsequent Commercialization in Ontario, Canada
- PMID: 36112372
- PMCID: PMC9482056
- DOI: 10.1001/jamanetworkopen.2022.31937
Changes in Emergency Department Visits for Cannabis Hyperemesis Syndrome Following Recreational Cannabis Legalization and Subsequent Commercialization in Ontario, Canada
Abstract
Importance: Prior research suggests that the legalization of recreational cannabis is associated with increases in cannabis hyperemesis syndrome (CHS), but it is unclear how cannabis commercialization (ie, greater retail store access as well as increased variety and potency of cannabis products) may be associated with these changes.
Objectives: To examine changes in the number and characteristics of CHS emergency department (ED) visits from before to after legalization of cannabis in Ontario, Canada.
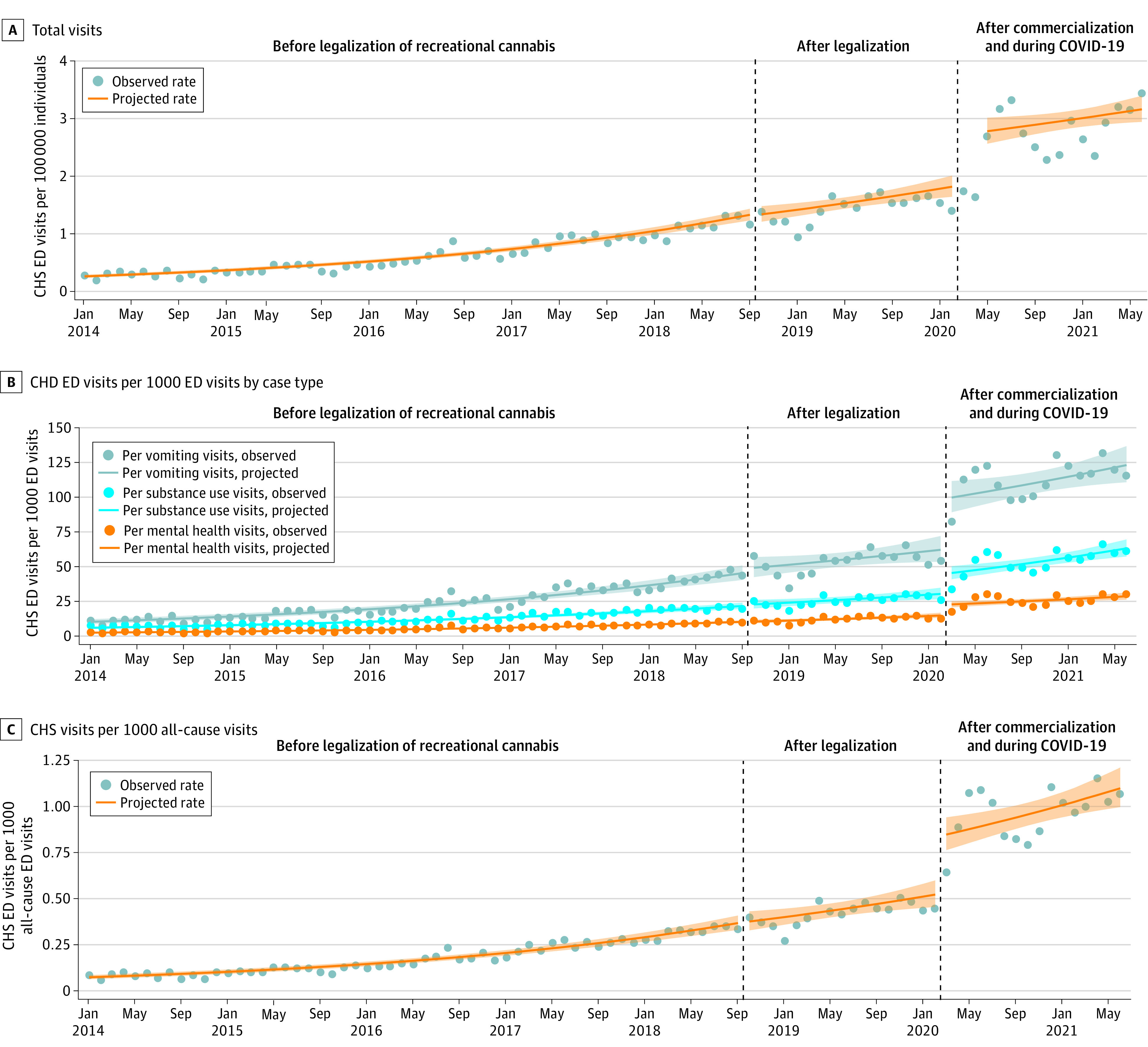
Design, setting, and participants: This repeated cross-sectional study used interrupted time-series analyses to examine immediate and gradual changes in ED visits for CHS in Ontario, Canada, during 3 time periods: prelegalization (January 2014-September 2018), legalization with product and retail store restrictions (October 2018-February 2020), and commercialization with new products and expanded stores, which coincided with the COVID-19 pandemic (March 2020-June 2021). Data were obtained from routinely collected and linked health administrative databases. All individuals aged at least 15 years and who were eligible for Ontario's Universal Health Coverage were included. Data were analyzed between March and July 2022.
Main outcomes and measures: Monthly counts of ED visits for CHS per capita.
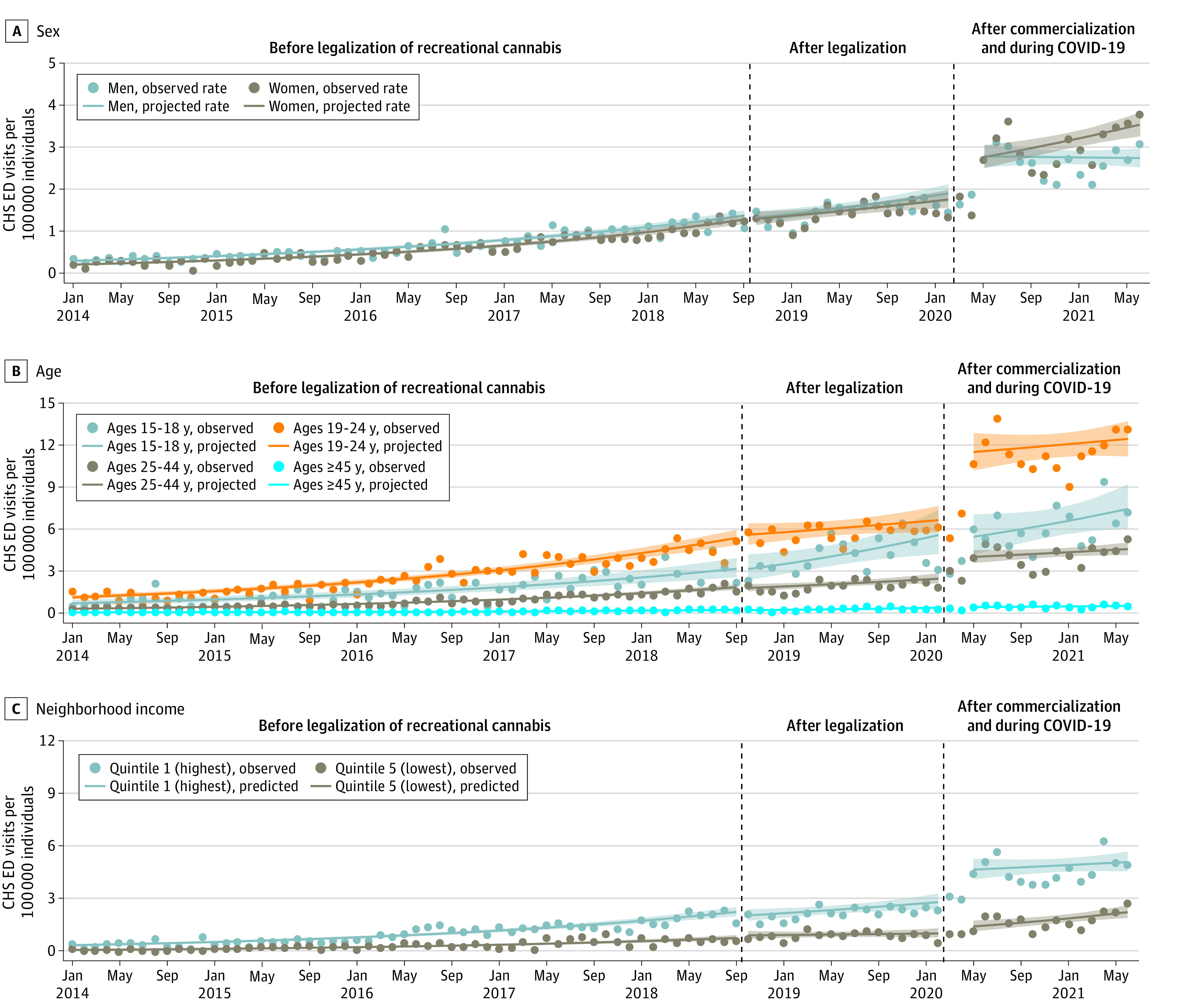
Results: There were 12 866 ED visits for CHS from 8140 individuals during the study. Overall, the mean (SD) age was 27.4 (10.5) years, with 2834 individuals (34.8%) aged 19 to 24 years, 4163 (51.5%) females, and 1353 individuals (16.6%) with a mental health ED visit or hospitalization in the 2 years before their first CHS ED visit. Nearly 10% of visits (1135 visits [8.8%]) led to hospital admissions. Monthly rates of CHS ED visits increased 13-fold during the 7.5-year study period, from 0.26 visits per 100 000 population in January 2014 to 3.43 visits per 100 000 population in June 2021. Legalization was not associated with an immediate or gradual change in rates of ED visits for CHS; however, commercialization during the COVID-19 pandemic period was associated with an immediate increase in rates of CHS ED visits (incidence rate ratio [IRR], 1.49; 95% CI, 1.31-1.70). During commercialization, rates of CHS ED visits increased more in women (IRR, 1.49; 95% CI, 1.16-1.92) and individuals older than the legal age of cannabis purchase (eg, age 19-24 years: IRR, 1.60; 95% CI, 1.19-2.16) than men (IRR, 1.08; 95% CI, 0.85-1.37) and individuals younger than the legal age of purchase (IRR, 0.78; 95% CI, 0.42-1.45).
Conclusions and relevance: This cross-sectional study found large increases in CHS ED visits during the period of time when the market commercialized and the COVID-19 pandemic occurred. Greater awareness of CHS symptoms by ED staff in regions where legal commercialized cannabis markets exist is indicated.
Conflict of interest statement
Figures
References
-
- Substance Abuse and Mental Health Services Administration . 2020 National Survey on Drug Use and Health: Table 1.1A: types of illicit drug use in lifetime, past year, and past month: among people aged 12 or older; numbers in thousands, 2019 and 2020. Accessed March 17, 2022. https://www.samhsa.gov/data/sites/default/files/reports/rpt35323/NSDUHDe...
-
- Health Canada . Statistic’s Canada. Canadian Alcohol and Drugs Survey (CADS): Summary of Results for 2019.; 2021. Accessed March 17, 2022. https://www.canada.ca/en/health-canada/services/canadian-alcohol-drugs-s...
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
