

Searching for a Consensus Among Inflammatory Bowel Disease Studies: A Systematic Meta-Analysis
- PMID: 36112501
- PMCID: PMC9825291
- DOI: 10.1093/ibd/izac194
Searching for a Consensus Among Inflammatory Bowel Disease Studies: A Systematic Meta-Analysis
Abstract
Background: Numerous studies have examined the gut microbial ecology of patients with Crohn's disease (CD) and ulcerative colitis, but inflammatory bowel disease-associated taxa and ecological effect sizes are not consistent between studies.
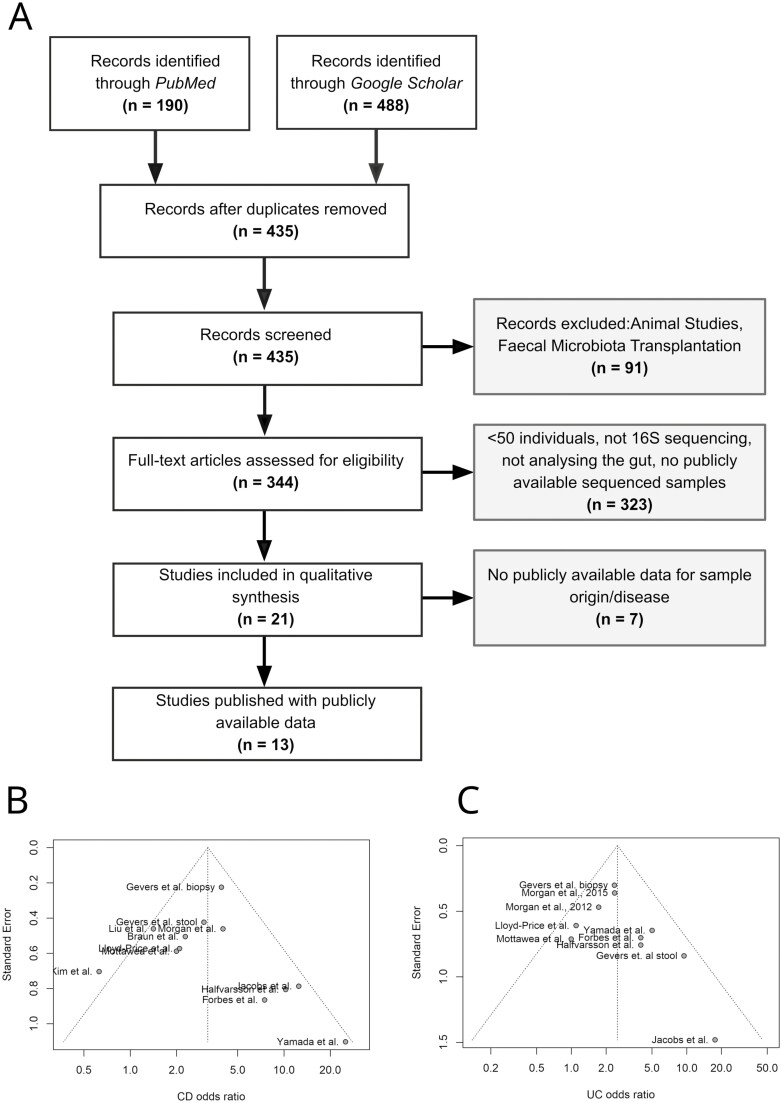
Methods: We systematically searched PubMed and Google Scholar and performed a meta-analysis of 13 studies to analyze how variables such as sample type (stool, biopsy, and lavage) affect results in inflammatory bowel disease gut microbiome studies, using uniform bioinformatic methods for all primary data.
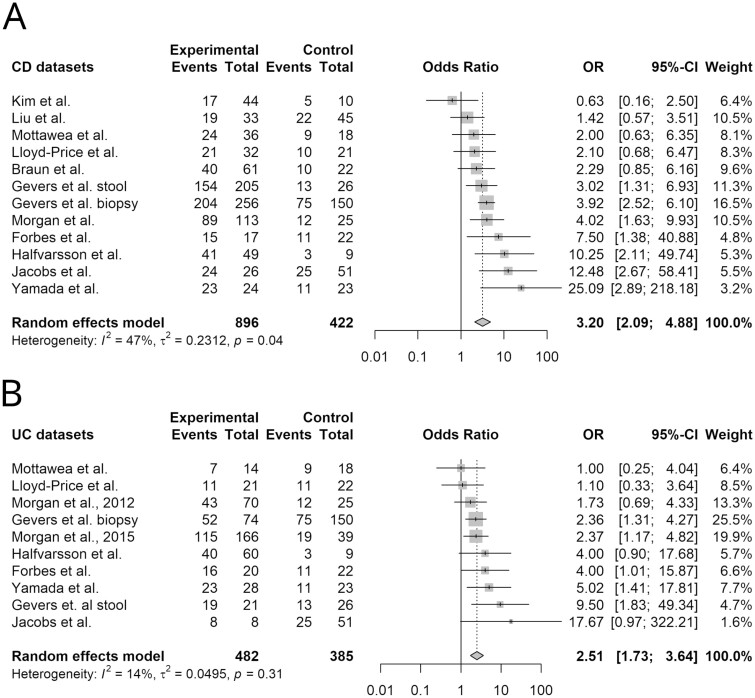
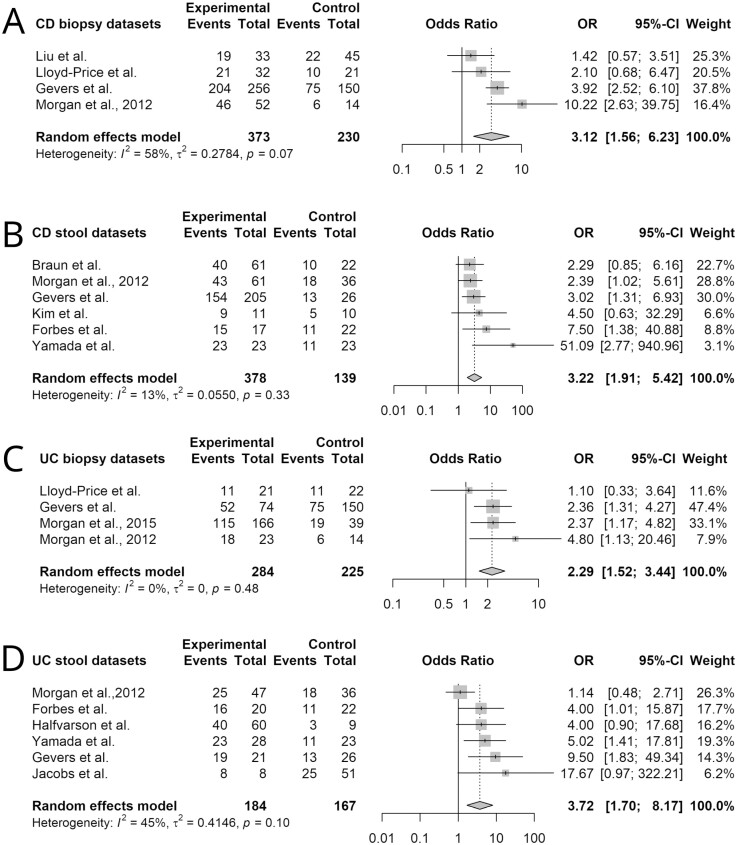
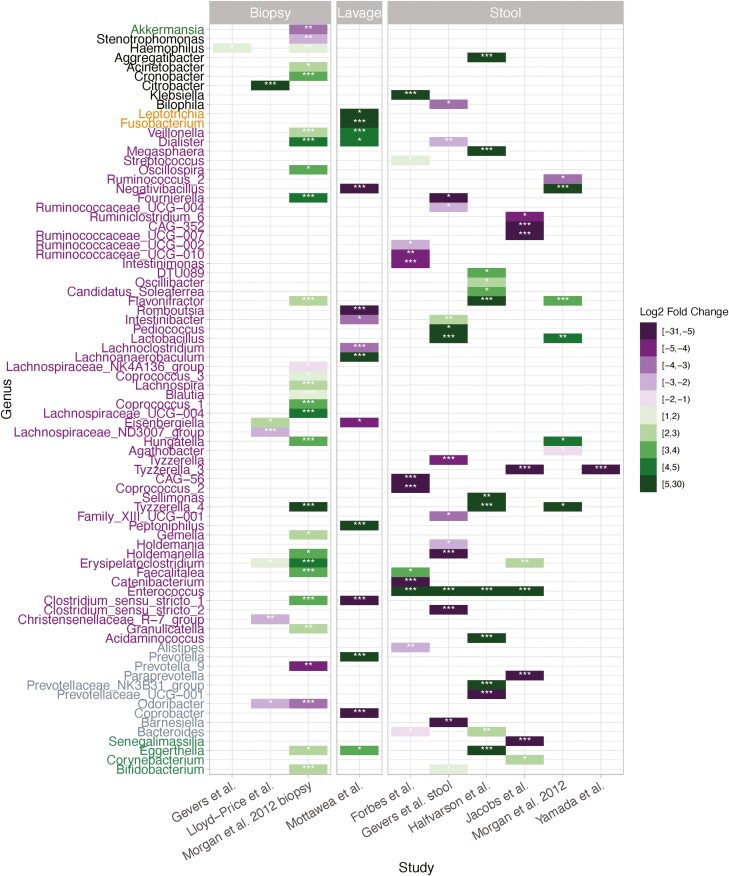
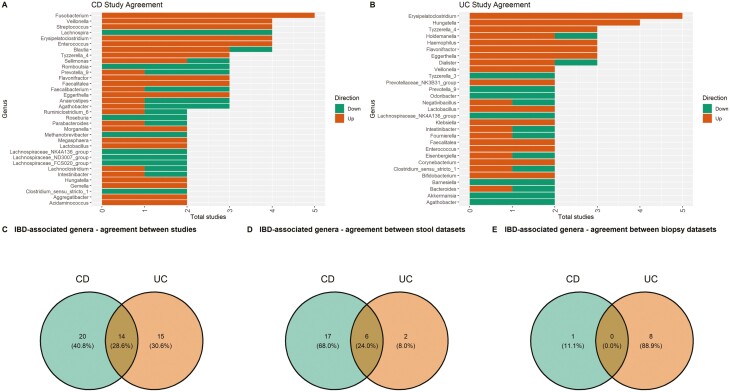
Results: Reduced alpha diversity was a consistent feature of both CD and ulcerative colitis but was more pronounced in CD. Disease contributed significantly variation in beta diversity in most studies, but effect size varied, and the effect of sample type was greater than the effect of disease. Fusobacterium was the genus most consistently associated with CD, but disease-associated genera were mostly inconsistent between studies. Stool studies had lower heterogeneity than biopsy studies, especially for CD.
Conclusions: Our results indicate that sample type variation is an important contributor to study variability that should be carefully considered during study design, and stool is likely superior to biopsy for CD studies due to its lower heterogeneity.
Keywords: CD; IBD; UC; alpha diversity; beta diversity; meta-analysis; microbiome; sequencing.
Plain language summary
To assess reproducibility in inflammatory bowel disease microbiome research, we performed a meta-analysis of 13 inflammatory bowel disease studies, measuring effects of disease and sample type. Crohn’s disease studies were more heterogeneous than ulcerative colitis studies, and sample type variation was a major contributor to inconsistency.
© 2022 Crohn’s & Colitis Foundation. Published by Oxford University Press on behalf of Crohn’s & Colitis Foundation.
Figures

Similar articles
-
Two-Sample Mendelian Randomization Analysis Investigates Causal Associations Between Gut Microbial Genera and Inflammatory Bowel Disease, and Specificity Causal Associations in Ulcerative Colitis or Crohn's Disease.Front Immunol. 2022 Jul 4;13:921546. doi: 10.3389/fimmu.2022.921546. eCollection 2022. Front Immunol. 2022. PMID: 35860271 Free PMC article.
-
Differentiating ulcerative colitis from Crohn disease in children and young adults: report of a working group of the North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition and the Crohn's and Colitis Foundation of America.J Pediatr Gastroenterol Nutr. 2007 May;44(5):653-74. doi: 10.1097/MPG.0b013e31805563f3. J Pediatr Gastroenterol Nutr. 2007. PMID: 17460505
-
Gut microbiota analyses of inflammatory bowel diseases from a representative Saudi population.BMC Gastroenterol. 2023 Jul 28;23(1):258. doi: 10.1186/s12876-023-02904-2. BMC Gastroenterol. 2023. PMID: 37507685 Free PMC article.
-
Morphologic criteria applicable to biopsy specimens for effective distinction of inflammatory bowel disease from other forms of colitis and of Crohn's disease from ulcerative colitis.Scand J Gastroenterol. 1999 Jan;34(1):55-67. doi: 10.1080/00365529950172844. Scand J Gastroenterol. 1999. PMID: 10048734
-
Conventional therapy for moderate to severe inflammatory bowel disease: A systematic literature review.World J Gastroenterol. 2019 Mar 7;25(9):1142-1157. doi: 10.3748/wjg.v25.i9.1142. World J Gastroenterol. 2019. PMID: 30863001 Free PMC article.
Cited by
-
Gut microbial and human genetic signatures of inflammatory bowel disease increase risk of comorbid mental disorders.NPJ Genom Med. 2024 Oct 29;9(1):52. doi: 10.1038/s41525-024-00440-w. NPJ Genom Med. 2024. PMID: 39472439 Free PMC article.
-
Microbiome Composition in Microscopic Colitis: A Systematic Review.Int J Mol Sci. 2023 Apr 10;24(8):7026. doi: 10.3390/ijms24087026. Int J Mol Sci. 2023. PMID: 37108189 Free PMC article.
-
Combining site-specific gut microbiome and mycobiome profiling with clinical indicators for effective management of pediatric Crohn's disease.iScience. 2025 Jul 18;28(8):113160. doi: 10.1016/j.isci.2025.113160. eCollection 2025 Aug 15. iScience. 2025. PMID: 40822348 Free PMC article.
-
Novel Insights into the Pathogenesis of Inflammatory Bowel Diseases.Biomedicines. 2025 Jan 26;13(2):305. doi: 10.3390/biomedicines13020305. Biomedicines. 2025. PMID: 40002718 Free PMC article. Review.
-
Mucosal Metabolomic Signatures in Chronic Colitis: Novel Insights into the Pathophysiology of Inflammatory Bowel Disease.Metabolites. 2023 Jul 23;13(7):873. doi: 10.3390/metabo13070873. Metabolites. 2023. PMID: 37512580 Free PMC article.
References
-
- Ng SC, Shi HY, Hamidi N, et al. . Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: a systematic review of population-based studies. Lancet 2017;390:2769-2778. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
