

Extensor hood injuries in elite boxers: injury characteristics, surgical technique and outcomes
- PMID: 36112963
- PMCID: PMC9727113
- DOI: 10.1177/17531934221123139
Extensor hood injuries in elite boxers: injury characteristics, surgical technique and outcomes
Abstract
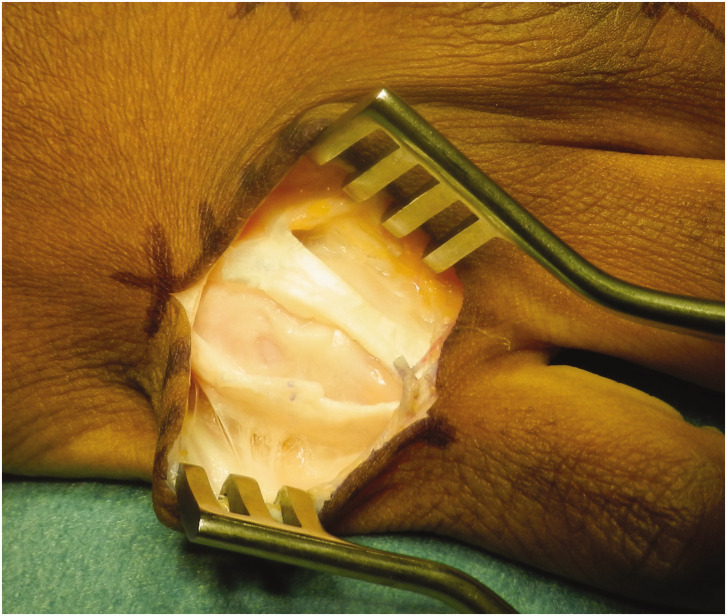
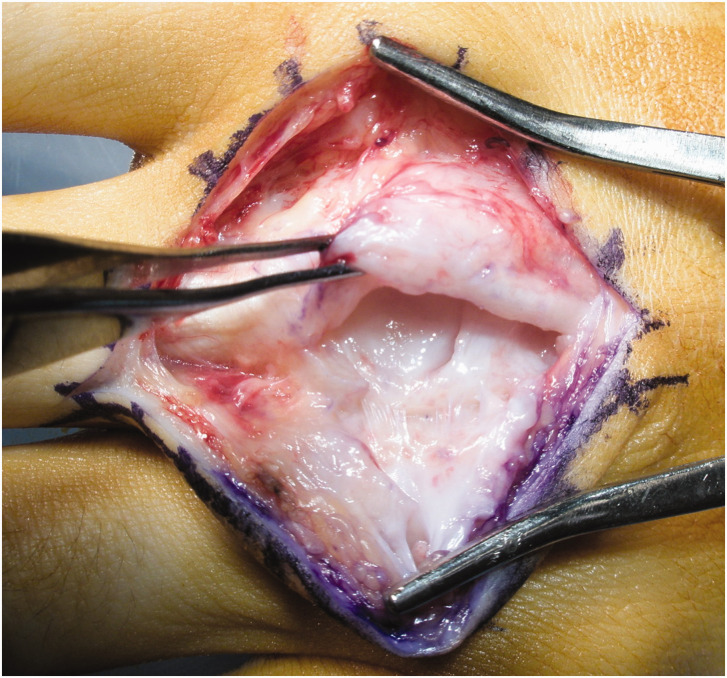
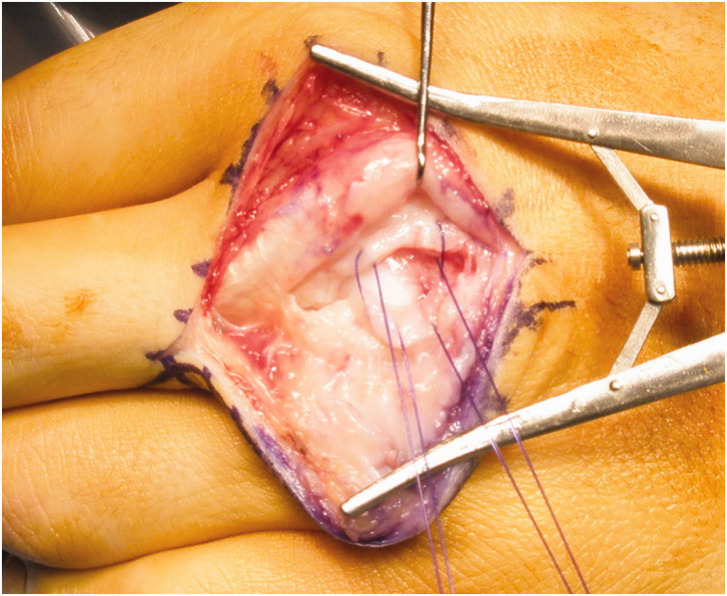
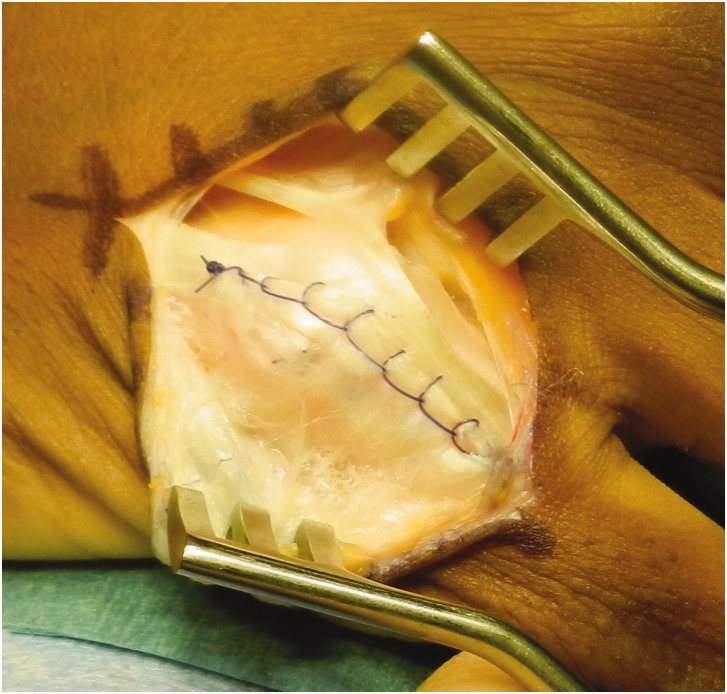
We describe our experience of managing extensor hood injuries in boxers (57 fingers). The diagnosis was mostly clinical, with imaging only if the diagnosis was equivocal. The middle (61%) and index (26%) digits were most frequently injured. On exploration, 26% had no hood tear, however all required tenolysis from the adherent capsule. Of 42 hood tears, 15 were central splits between adjacent extensor tendons in the index or little fingers,15 tears were on the ulna side of the extensor tendon and 12 tears were on the radial side. A pseudobursa was encountered in 35%, capsular tears in 28% and chondral injury in one patient. Longitudinal curved metacarpophalangeal joint incisions were used, with hood repair performed in flexion using a locked running suture. Mean postoperative metacarpophalangeal joint flexion was 90°. Ninety-eight per cent returned to the same level of boxing at a mean of 8 months (range 1-24) from surgery. One finger was revised for re-rupture 6 months later. A reproducible technique for treating these injuries is described, with patients able to return to boxing with little risk of complications.Level of evidence: IV.
Keywords: Extensor hood injury; elite athlete; outcomes; return to sport; surgical repair.
Conflict of interest statement
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures

Similar articles
-
[Closed injuries of the extensor hood of the metacarpophalangeal joint].Unfallchirurgie. 1997 Dec;23(6):262-6. doi: 10.1007/BF02628923. Unfallchirurgie. 1997. PMID: 9483789 Review. German.
-
Boxer's knuckle in the professional athlete.Am J Sports Med. 2000 Nov-Dec;28(6):879-82. doi: 10.1177/03635465000280061701. Am J Sports Med. 2000. PMID: 11101112
-
Boxer's knuckle--dorsal capsular rupture of the metacarpophalangeal joint of a finger.J Hand Surg Am. 1989 Mar;14(2 Pt 1):229-36. doi: 10.1016/0363-5023(89)90011-7. J Hand Surg Am. 1989. PMID: 2703667
-
Extensor retinaculum graft for chronic boxer's knuckle.J Hand Surg Am. 2006 Jul-Aug;31(6):947-51. doi: 10.1016/j.jhsa.2006.02.027. J Hand Surg Am. 2006. PMID: 16843154
-
Extensor tendon centralization at the metacarpophalangeal joint: surgical technique.J Hand Surg Am. 2010 Jul;35(7):1194-7. doi: 10.1016/j.jhsa.2010.04.029. J Hand Surg Am. 2010. PMID: 20610064 Review.
Cited by
-
New Insights into Boxer's Knuckle Injury of the Little Finger.J Clin Med. 2023 Dec 21;13(1):46. doi: 10.3390/jcm13010046. J Clin Med. 2023. PMID: 38202053 Free PMC article.
-
WALANT surgery of the hand: state of the art.EFORT Open Rev. 2024 May 10;9(5):349-356. doi: 10.1530/EOR-24-0033. EFORT Open Rev. 2024. PMID: 38726975 Free PMC article. Review.
-
Boxer's knuckle: Sonographic anatomy and assessment of sagittal band tears of the dorsal hood.Australas J Ultrasound Med. 2023 Oct 12;26(4):216-229. doi: 10.1002/ajum.12363. eCollection 2023 Nov. Australas J Ultrasound Med. 2023. PMID: 38098620 Free PMC article. No abstract available.
References
-
- Arai K, Toh S, Nakahara K, Nishikawa S, Harata S. Treatment of soft tissue injuries to the dorsum of the metacarpophalangeal joint (Boxer's knuckle). J Hand Surg Br. 2002, 27: 90–5. - PubMed
-
- Bents RT, Metz JP, Topper SM. Traumatic extensor tendon dislocation in a boxer: a case study. Med Sci Sports Exerc. 2003, 35: 1645–7. - PubMed
-
- Hame SL, Melone CP. Boxer's knuckle in the professional athlete. Am J Sports Med. 2000, 28: 879–82. - PubMed
-
- Lin JD, Strauch RJ. Closed soft tissue extensor mechanism injuries (mallet, boutonniere, and sagittal band). J Hand Surg Am. 2014, 39: 1005–11. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
