

Feasibility of measles and rubella vaccination programmes for disease elimination: a modelling study
- PMID: 36113527
- PMCID: PMC9557212
- DOI: 10.1016/S2214-109X(22)00335-7
Feasibility of measles and rubella vaccination programmes for disease elimination: a modelling study
Abstract
Background: Marked reductions in the incidence of measles and rubella have been observed since the widespread use of the measles and rubella vaccines. Although no global goal for measles eradication has been established, all six WHO regions have set measles elimination targets. However, a gap remains between current control levels and elimination targets, as shown by large measles outbreaks between 2017 and 2019. We aimed to model the potential for measles and rubella elimination globally to inform a WHO report to the 73rd World Health Assembly on the feasibility of measles and rubella eradication.
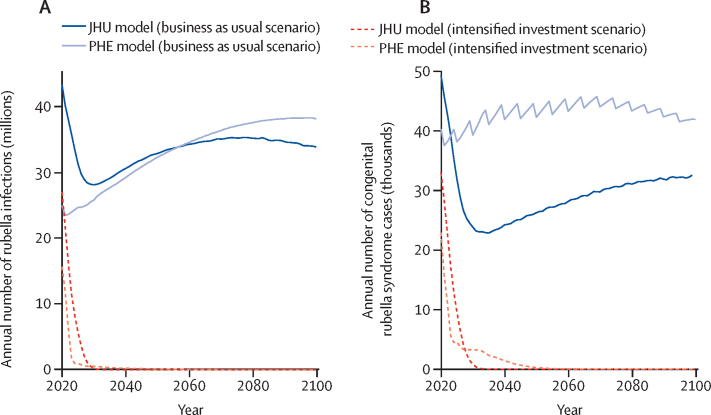
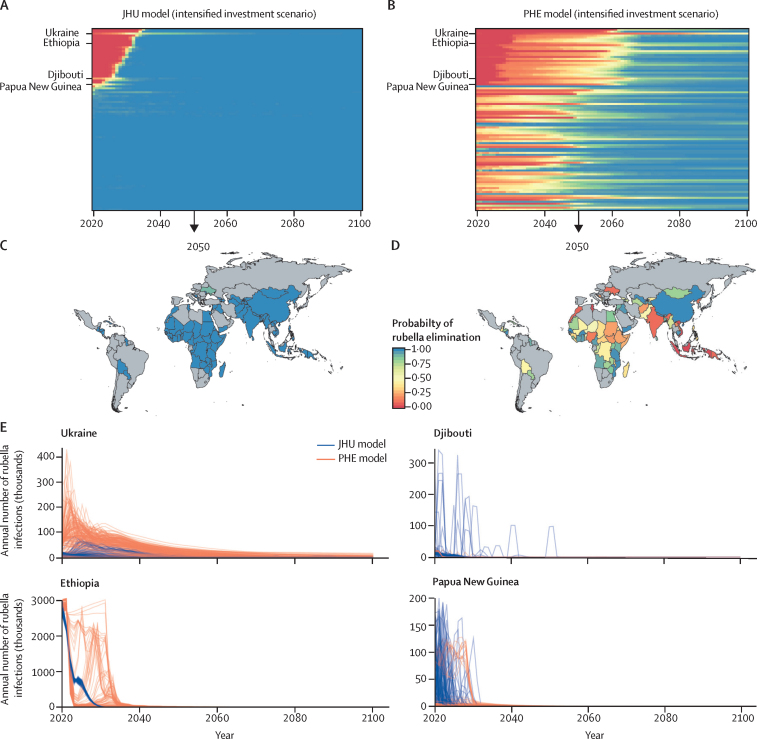
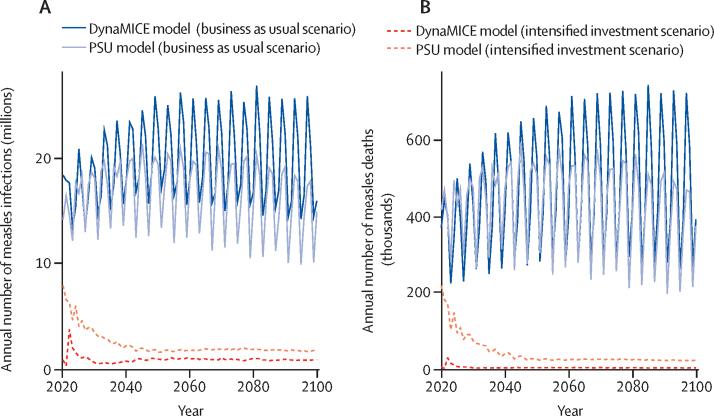
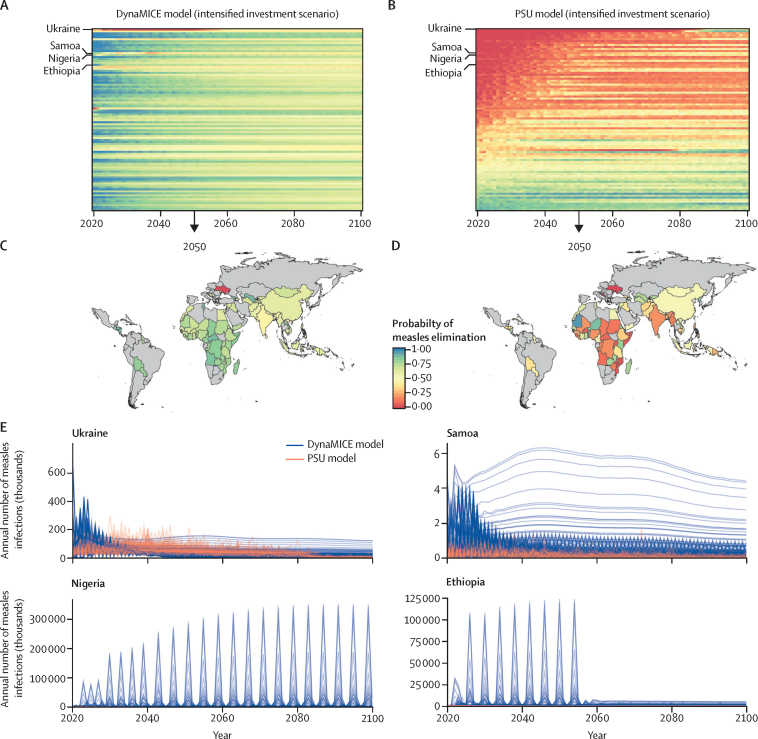
Methods: In this study, we modelled the probability of measles and rubella elimination between 2020 and 2100 under different vaccination scenarios in 93 countries of interest. We evaluated measles and rubella burden and elimination across two national transmission models each (Dynamic Measles Immunisation Calculation Engine [DynaMICE], Pennsylvania State University [PSU], Johns Hopkins University, and Public Health England models), and one subnational measles transmission model (Institute for Disease Modeling model). The vaccination scenarios included a so-called business as usual approach, which continues present vaccination coverage, and an intensified investment approach, which increases coverage into the future. The annual numbers of infections projected by each model, country, and vaccination scenario were used to explore if, when, and for how long the infections would be below a threshold for elimination.
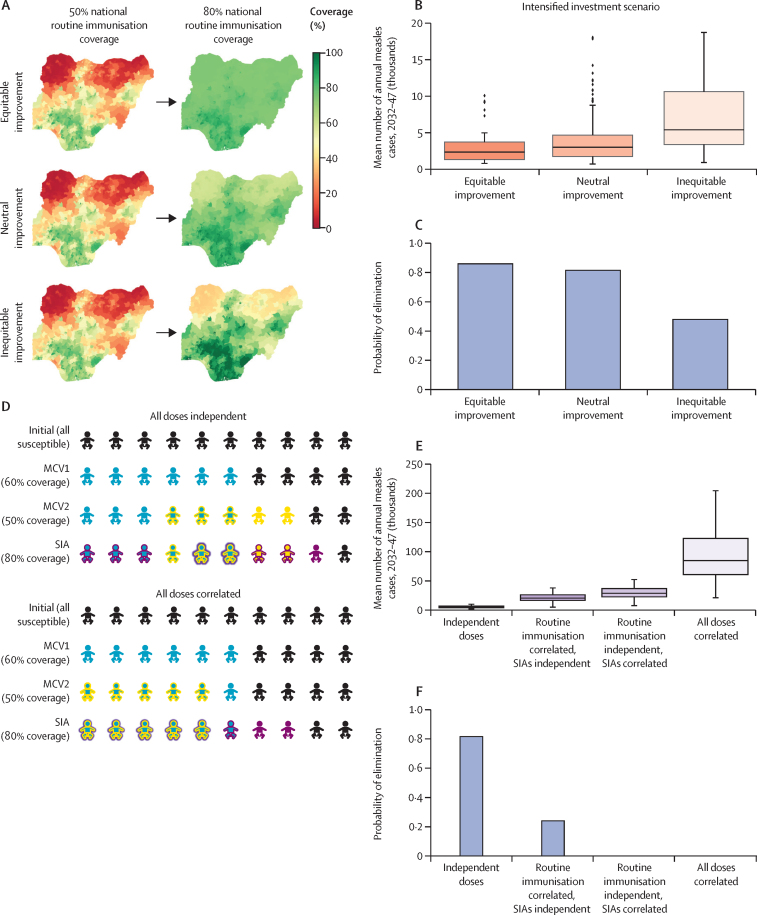
Findings: The intensified investment scenario led to large reductions in measles and rubella incidence and burden. Rubella elimination is likely to be achievable in all countries and measles elimination is likely in some countries, but not all. The PSU and DynaMICE national measles models estimated that by 2050, the probability of elimination would exceed 75% in 14 (16%) and 36 (39%) of 93 modelled countries, respectively. The subnational model of measles transmission highlighted inequity in routine coverage as a likely driver of the continuance of endemic measles transmission in a subset of countries.
Interpretation: To reach regional elimination goals, it will be necessary to innovate vaccination strategies and technologies that increase spatial equity of routine vaccination, in addition to investing in existing surveillance and outbreak response programmes.
Funding: WHO, Gavi, the Vaccine Alliance, US Centers for Disease Control and Prevention, and the Bill & Melinda Gates Foundation.
Copyright © 2022 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests MJ, MF, AKW, ST, and JL report grants from the Bill & Melinda Gates Foundation and Gavi, the Vaccine Alliance. EV reports grants from WHO. MJ and MF report grants from WHO. JL and MF report grants from the US Centers for Disease Control and Prevention (CDC) and National Institutes of Health. MF additionally receives grants from the National Science Foundation. SER and MJ are members of the WHO Strategic Group of Experts on Immunization (SAGE) working group on measles and rubella. SER is acting Chair of the Measles and Rubella Initiative and a member of the Measles and Rubella Post Elimination Regional Monitoring and Re-verification Commission of Pan American Health Organization and The Regional Verification Commission for Measles and Rubella Elimination in the Eastern Mediterranean Region. KM is an employee of the Institute of Disease Modeling and the Bill & Melinda Gates Foundation. CB reports grants from WHO, and is currently a contract employee of Diversant, on contract to Merck Research Laboratories. TP, DK, JKK, LKK, HS, SS, KK, PK, and BL declare no competing interests. The findings and conclusions in this Article are those of the authors and do not necessarily represent the views of the US CDC. The views expressed are those of the authors and not necessarily those of the Vaccine Impact Modelling Consortium or its funders.
Figures
Comment in
-
Investing in global measles and rubella elimination is needed to avert deaths and advance health equity.Lancet Glob Health. 2022 Oct;10(10):e1363-e1364. doi: 10.1016/S2214-109X(22)00388-6. Lancet Glob Health. 2022. PMID: 36113510 Free PMC article. No abstract available.
References
-
- WHO Introduction of rubella vaccine. 2021. https://immunizationdata.who.int/pages/vaccine-intro-by-antigen/rubella....
-
- Kirby T. Rubella is eliminated from the Americas. Lancet Infect Dis. 2015;15:768–769. - PubMed
-
- WHO Global measles and rubella: strategic plan 2012–2020. 2012. https://www.who.int/publications/i/item/9789241503396
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
