

Comparing one dose of HPV vaccine in girls aged 9-14 years in Tanzania (DoRIS) with one dose of HPV vaccine in historical cohorts: an immunobridging analysis of a randomised controlled trial
- PMID: 36113532
- PMCID: PMC9638025
- DOI: 10.1016/S2214-109X(22)00306-0
Comparing one dose of HPV vaccine in girls aged 9-14 years in Tanzania (DoRIS) with one dose of HPV vaccine in historical cohorts: an immunobridging analysis of a randomised controlled trial
Abstract
Background: Human papillomavirus (HPV) vaccines are given as a two-dose schedule in children aged 9-14 years, or as three doses in older individuals. We compared antibody responses after one dose of HPV vaccine in the Dose Reduction Immunobridging and Safety Study (DoRIS), a randomised trial of different HPV vaccine schedules in Tanzania, to those from two observational HPV vaccine trials that found high efficacy of one dose up to 11 years against HPV16 and HPV18 (Costa Rica Vaccine Trial [CVT] and Institutional Agency for Research on Cancer [IARC] India trial).
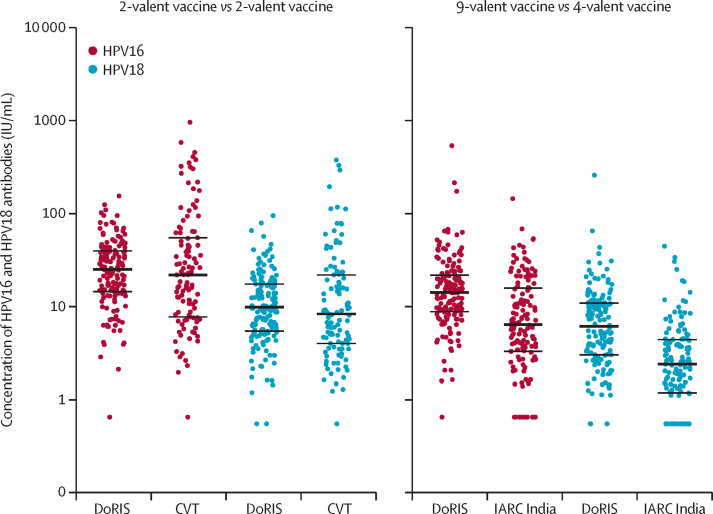
Methods: In this immunobridging analysis of an open-label randomised controlled trial, girls were recruited from 54 government schools in Mwanza, Tanzania, into the DoRIS trial. Girls were eligible if they were aged 9-14 years, healthy, and HIV negative. Participants were randomly assigned (1:1:1:1:1:1), using permutated block sizes of 12, 18, and 24, to one, two, or three doses of the 2-valent vaccine (Cervarix, GSK Biologicals, Rixensart, Belgium) or the 9-valent vaccine (Gardasil 9, Sanofi Pasteur MSD, Lyon, France). For this immunobridging analysis, the primary objective was to compare geometric mean concentrations (GMCs) at 24 months after one dose in the per-protocol population compared with in historical cohorts: the one-dose 2-valent vaccine group in DoRIS was compared with recipients of the 2-valent vaccine Cervarix from CVT and the one-dose 9-valent vaccine group in DoRIS was compared with recipients of the 4-valent vaccine Gardasil (Merck Sharp & Dohme, Whitehouse Station, NJ, USA) from the IARC India trial. Samples were tested together with virus-like particle ELISA for HPV16 and HPV18 IgG antibodies. Non-inferiority of GMC ratios (DoRIS trial vs historical cohort) was predefined as when the lower bound of the 95% CI was greater than 0·50. This study is registered with ClinicalTrials.gov, NCT02834637.
Findings: Between Feb 23, 2017, and Jan 6, 2018, we screened 1002 girls for eligibility, of whom 930 were enrolled into DoRIS and 155 each were assigned to one dose, two doses, or three doses of 2-valent vaccine, or one dose, two doses, or three doses of 9-valent vaccine. 154 (99%) participants in the one-dose 2-valent vaccine group (median age 10 years [IQR 9-12]) and 152 (98%) in the one-dose 9-valent vaccine group (median age 10 years [IQR 9-12]) were vaccinated and attended the 24 month visit, and so were included in the analysis. 115 one-dose recipients from the CVT (median age 21 years [19-23]) and 139 one-dose recipients from the IARC India trial (median age 14 years [13-16]) were included in the analysis. At 24 months after vaccination, GMCs for HPV16 IgG antibodies were 22·9 international units (IU) per mL (95% CI 19·9-26·4; n=148) for the DoRIS 2-valent vaccine group versus 17·7 IU/mL (13·9-22·5; n=97) for the CVT (GMC ratio 1·30 [95% CI 1·00-1·68]) and 13·7 IU/mL (11·9-15·8; n=145) for the DoRIS 9-valent vaccine group versus 6·7 IU/mL (5·5-8·2; n=131) for the IARC India trial (GMC ratio 2·05 [1·61-2·61]). GMCs for HPV18 IgG antibodies were 9·9 IU/mL (95% CI 8·5-11·5: n=141) for the DoRIS 2-valent vaccine group versus 8·0 IU/mL (6·4-10·0; n=97) for the CVT trial (GMC ratio 1·23 [95% CI 0·95-1·60]) and 5·7 IU/mL (4·9-6·8; n=136) for the DoRIS 9-valent vaccine group versus 2·2 IU/mL (1·9-2·7; n=129) for the IARC India trial (GMC ratio 2·12 [1·59-2·83]). Non-inferiority of antibody GMCs was met for each vaccine for both HPV16 and HPV18.
Interpretation: One dose of HPV vaccine in young girls might provide sufficient protection against persistent HPV infection. A one-dose schedule would reduce costs, simplify vaccine delivery, and expand access to the vaccine.
Funding: UK Department for International Development/UK Medical Research Council/Wellcome Trust Joint Global Health Trials Scheme, The Bill & Melinda Gates Foundation, and the US National Cancer Institute.
Translation: For the KiSwahili translation of the abstract see Supplementary Materials section.
Copyright © 2022 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests KB, HW, and DW-J report a grant from Merck for a new study of single-dose HPV vaccination in males in Tanzania, unrelated to this submitted work. PB, ARK, JTS, HW, and DW-J are members of the Single Dose HPV Vaccine Evaluation Consortium, coordinated by PATH and funded by the Bill & Melinda Gates Foundation. PB reports a grant from GSK Biologicals for a previous study on safety and immunogenicity of Cervarix in India unrelated to this submitted work during his previous position at Chittaranjan National Cancer Institute, Kolkata, India. DW-J reports a grant from GSK Biologicals in 2007 for a previous on safety and immunogenicity of Cervarix in Tanzania, unrelated to this submitted work. JTS reports that he was a named inventor on US Government-owned HPV vaccine patents that were licensed to GlaxoSmithKline and Merck and for which the US National Cancer Institute (NCI) previously received licensing fees. NCI's licenses have now expired but JTS was previously entitled to royalties to a specified amount, as determined by federal law governing technological transfer activities by US Government employees. All other authors declare no competing interests.
Figures
Comment in
-
HPV vaccines: when one plus one equals three.Lancet Glob Health. 2022 Oct;10(10):e1373-e1374. doi: 10.1016/S2214-109X(22)00373-4. Lancet Glob Health. 2022. PMID: 36113514 No abstract available.
References
-
- WHO . World Health Organization; Geneva: Nov 17, 2020. Global strategy to accelerate the elimination of cervical cancer as a public health problem.https://www.who.int/publications/i/item/9789240014107
-
- Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71:209–249. - PubMed
-
- Bruni L, Saura-Lázaro A, Montoliu A, et al. HPV vaccination introduction worldwide and WHO and UNICEF estimates of national HPV immunization coverage 2010–2019. Prev Med. 2021;144 - PubMed
-
- Meites E, Kempe A, Markowitz LE. Use of a 2-dose schedule for human papillomavirus vaccination - updated recommendations of the Advisory Committee on Immunization Practices. MMWR Morb Mortal Wkly Rep. 2016;65:1405–1408. - PubMed
-
- Gallagher KE, LaMontagne DS, Watson-Jones D. Status of HPV vaccine introduction and barriers to country uptake. Vaccine. 2018;36(32 Pt A):4761–4767. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
