

Th17 Cell-Derived Amphiregulin Promotes Colitis-Associated Intestinal Fibrosis Through Activation of mTOR and MEK in Intestinal Myofibroblasts
- PMID: 36113570
- PMCID: PMC9772145
- DOI: 10.1053/j.gastro.2022.09.006
Th17 Cell-Derived Amphiregulin Promotes Colitis-Associated Intestinal Fibrosis Through Activation of mTOR and MEK in Intestinal Myofibroblasts
Abstract
Background & aims: Intestinal fibrosis is a significant complication of Crohn's disease (CD). Gut microbiota reactive Th17 cells are crucial in the pathogenesis of CD; however, how Th17 cells induce intestinal fibrosis is still not completely understood.
Methods: In this study, T-cell transfer model with wild-type (WT) and Areg-/- Th17 cells and dextran sulfate sodium (DSS)-induced chronic colitis model in WT and Areg-/- mice were used. CD4+ T-cell expression of AREG was determined by quantitative reverse-transcriptase polymerase chain reaction and enzyme-linked immunosorbent assay. The effect of AREG on proliferation/migration/collagen expression in human intestinal myofibroblasts was determined. AREG expression was assessed in healthy controls and patients with CD with or without intestinal fibrosis.
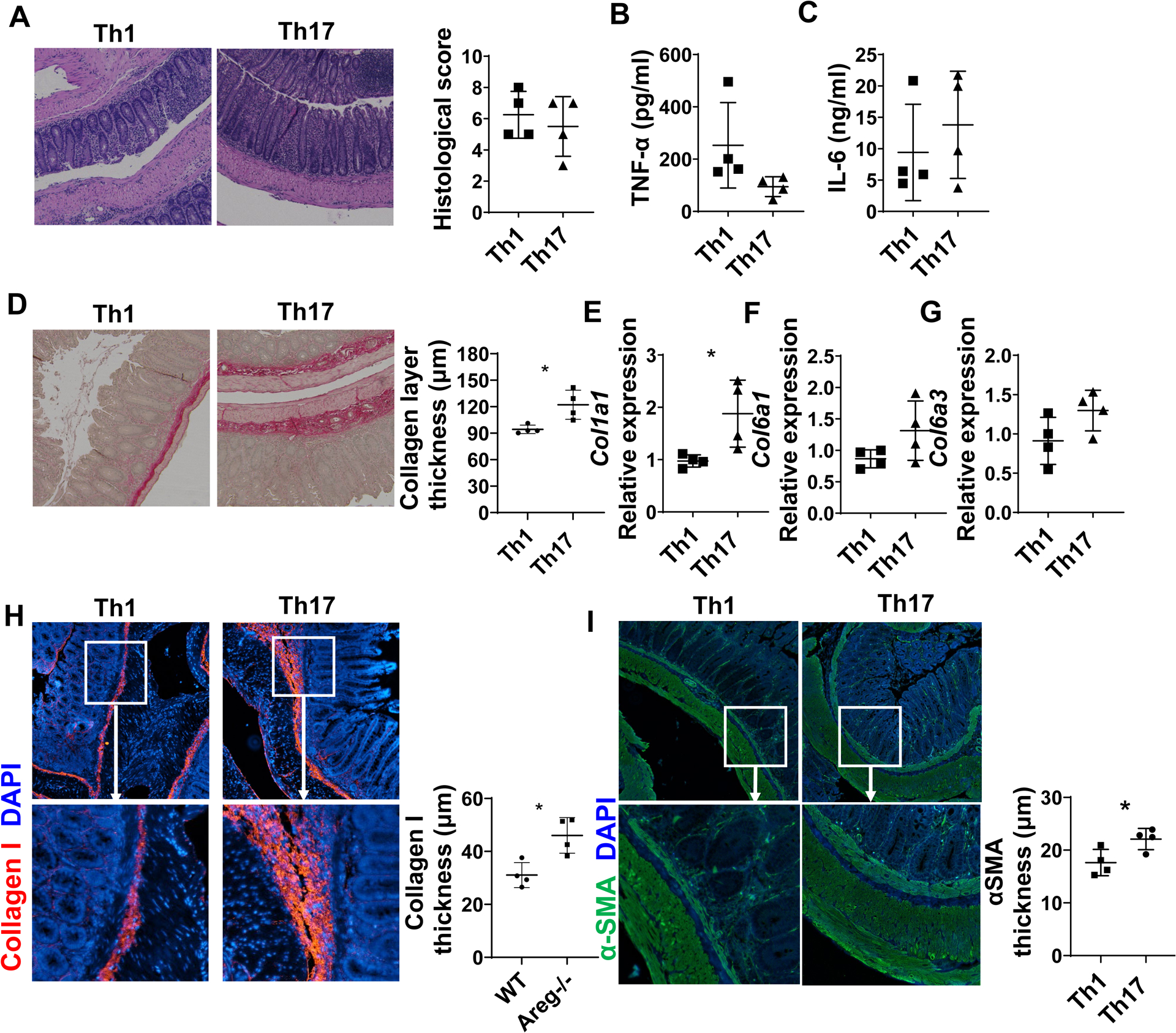
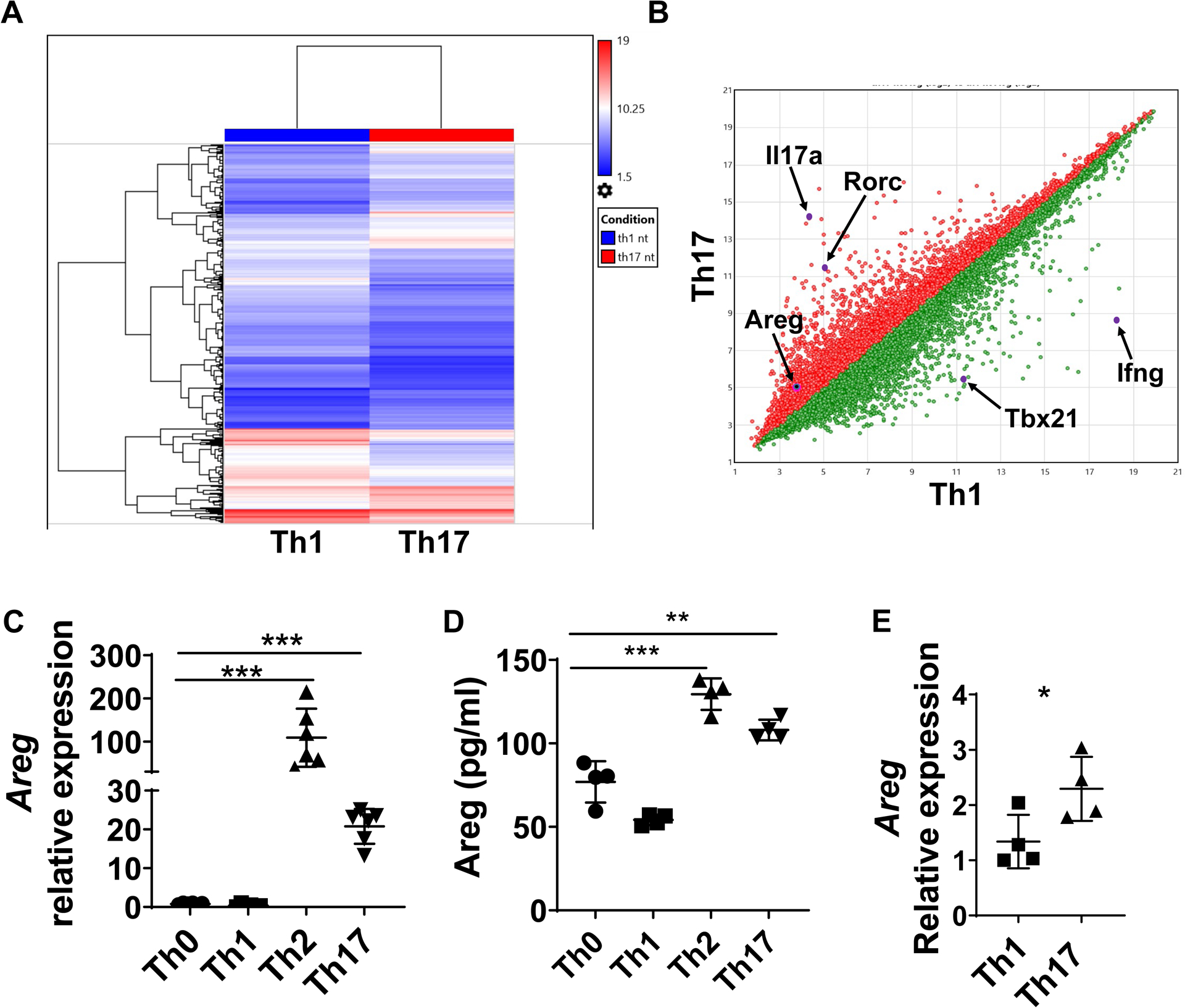
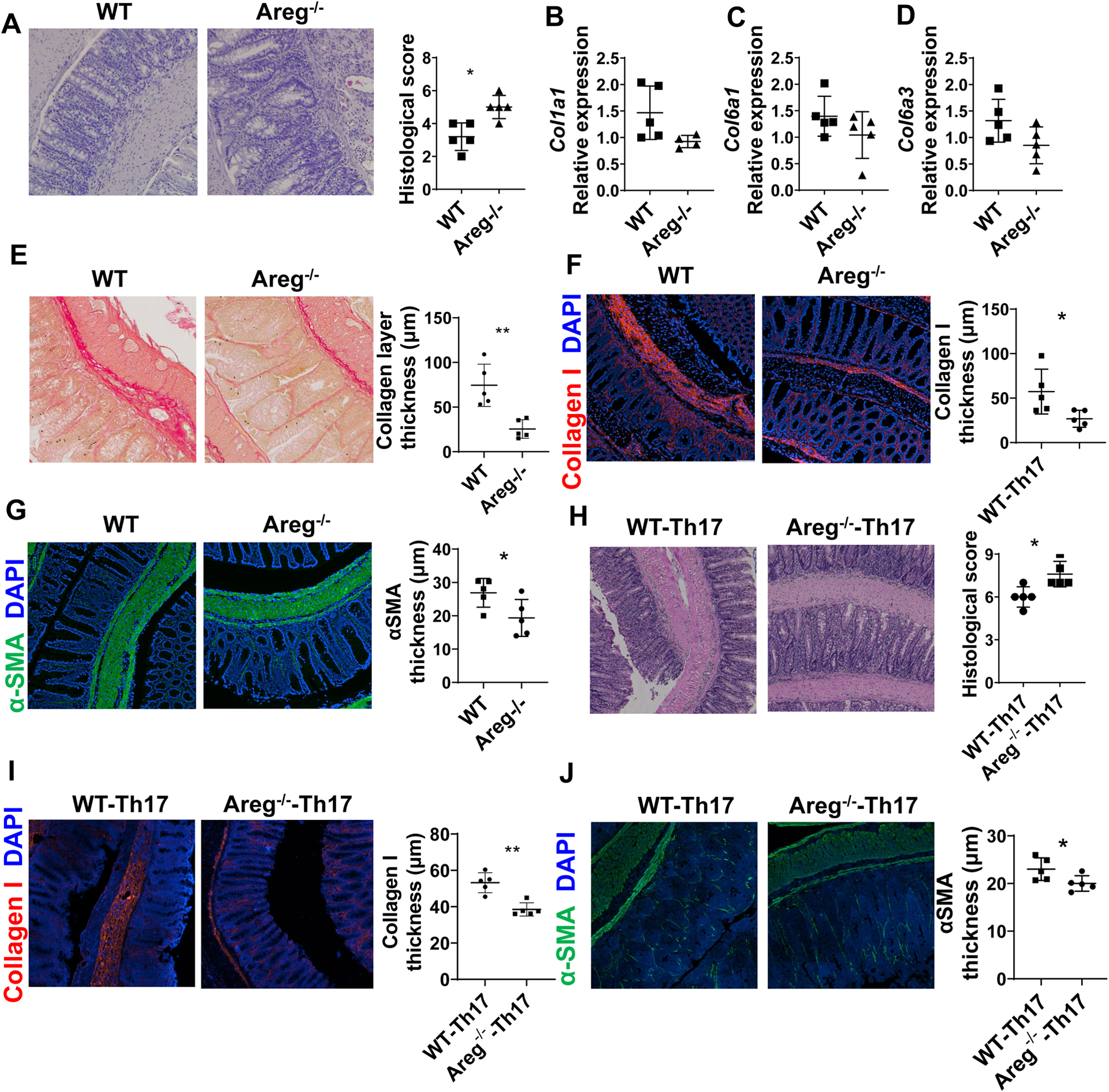
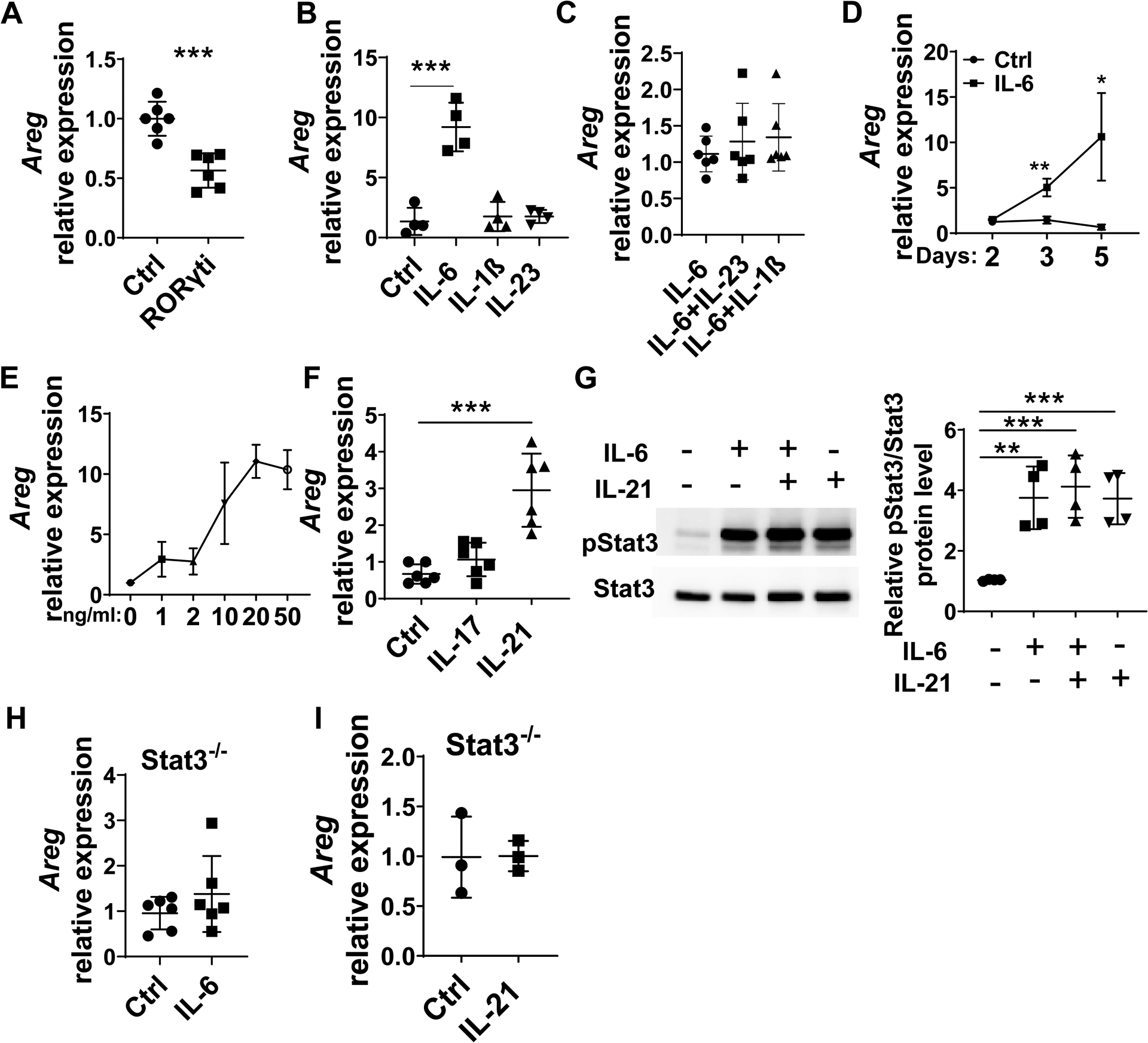
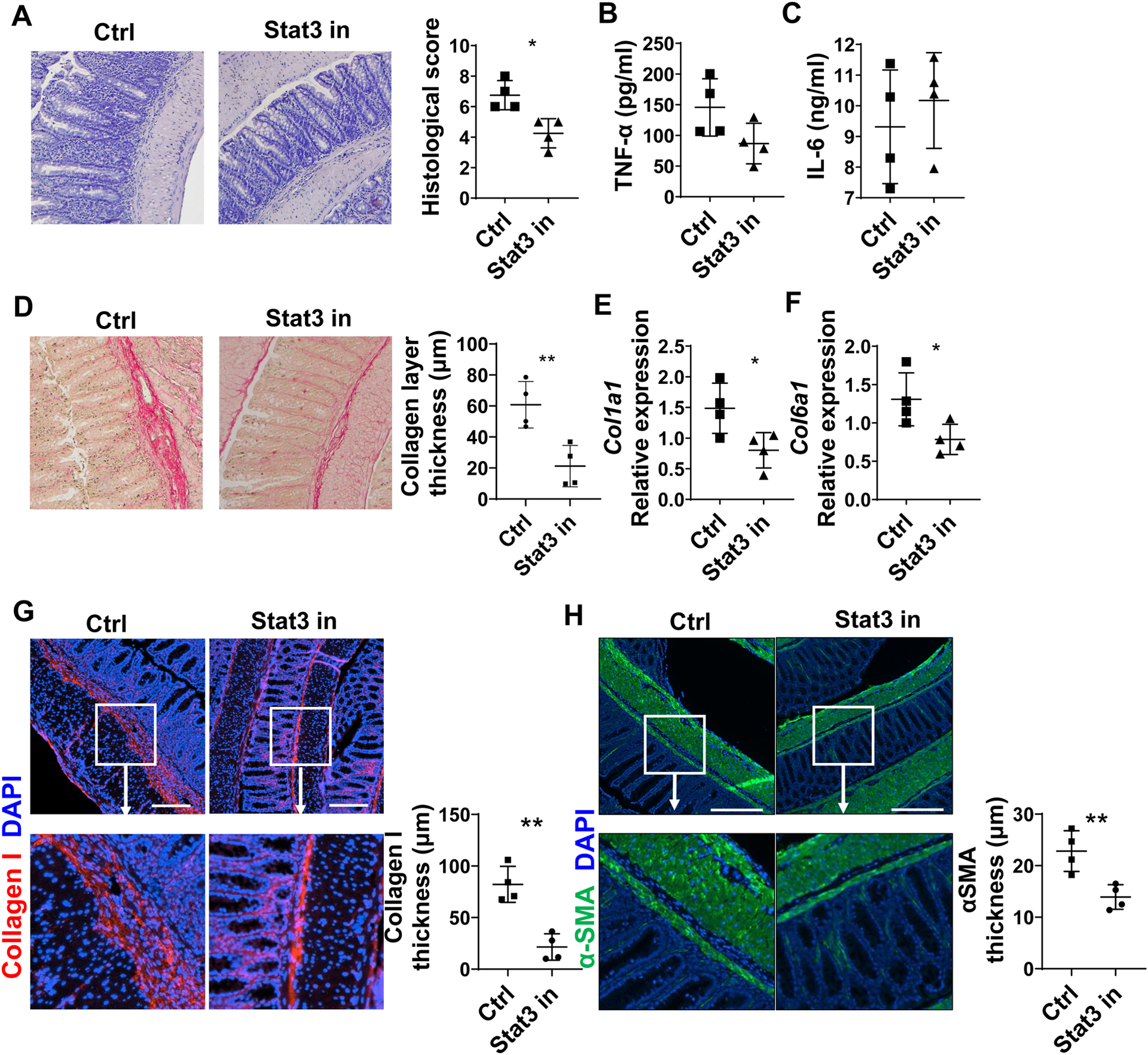
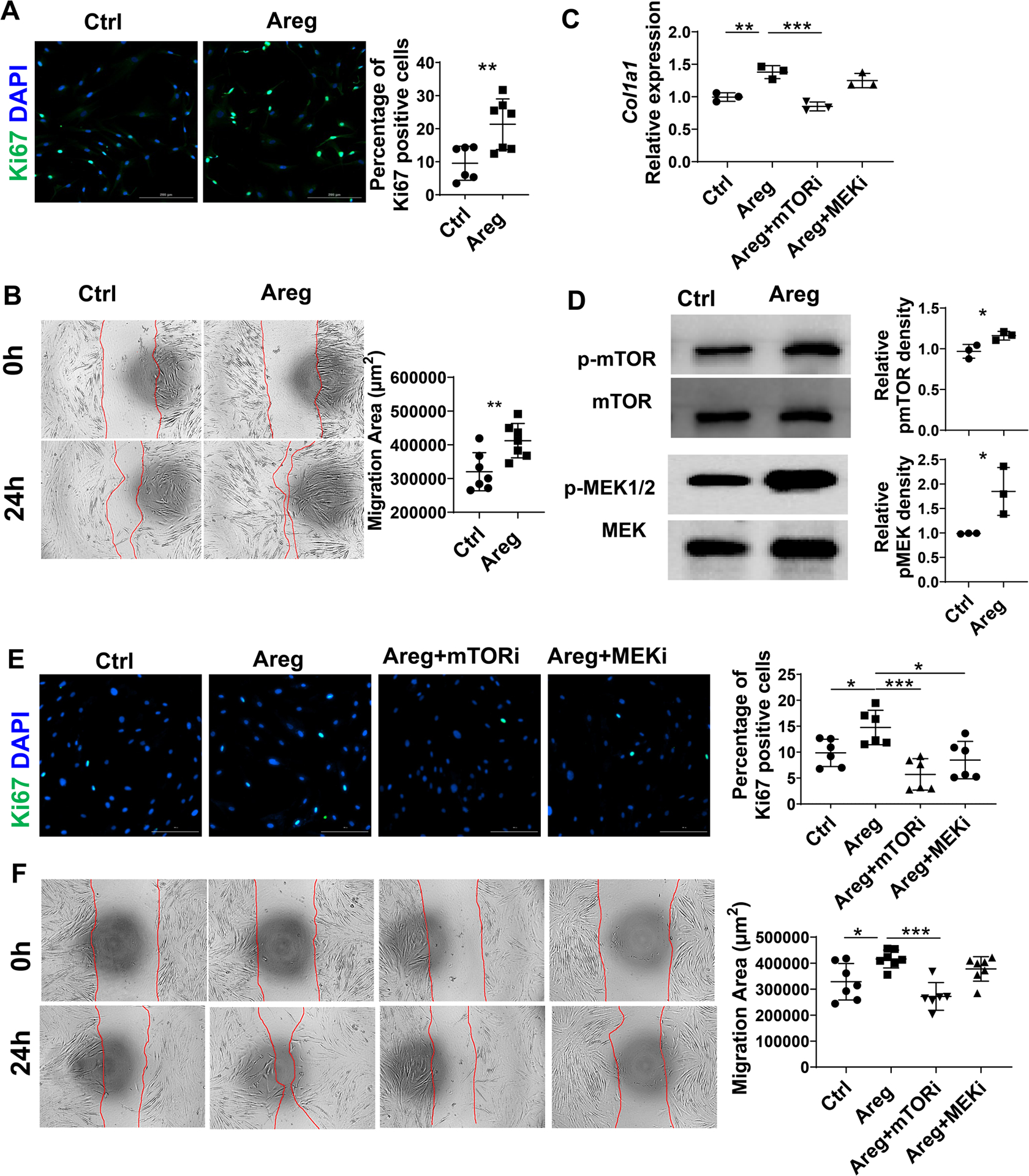
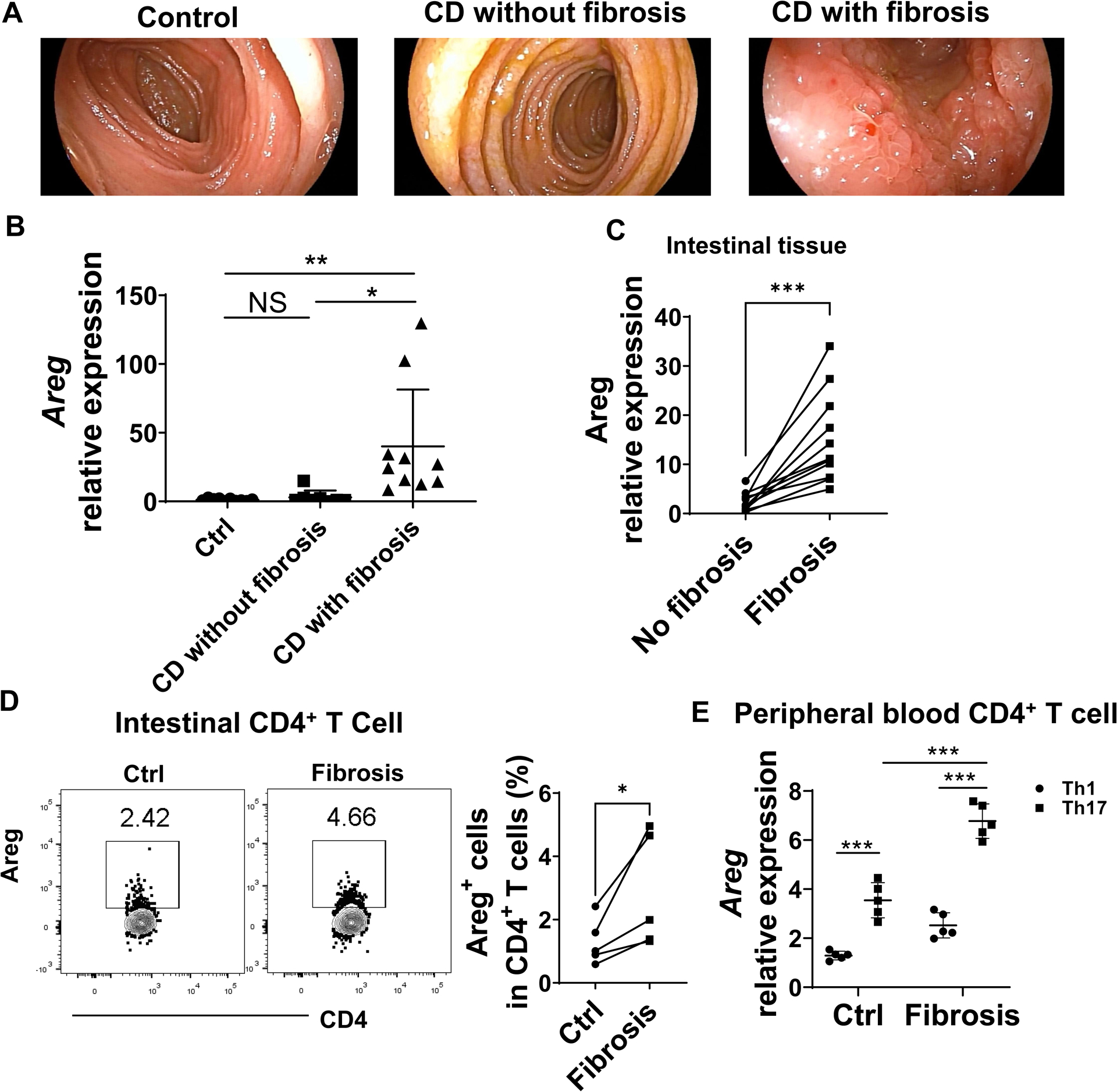
Results: Although Th1 and Th17 cells induced intestinal inflammation at similar levels when transferred into Tcrβxδ-/- mice, Th17 cells induced more severe intestinal fibrosis. Th17 cells expressed higher levels of AREG than Th1 cells. Areg-/- mice developed less severe intestinal fibrosis compared with WT mice on DSS insults. Transfer of Areg-/- Th17 cells induced less severe fibrosis in Tcrβxδ-/- mice compared with WT Th17 cells. Interleukin (IL)6 and IL21 promoted AREG expression in Th17 cells by activating Stat3. Stat3 inhibitor suppressed Th17-induced intestinal fibrosis. AREG promoted human intestinal myofibroblast proliferation, motility, and collagen I expression, which was mediated by activating mammalian target of rapamycin and MEK. AREG expression was increased in intestinal CD4+ T cells in fibrotic sites compared with nonfibrotic sites from patients with CD.
Conclusions: These findings reveal that Th17-derived AREG promotes intestinal fibrotic responses in experimental colitis and human patients with CD. Thereby, AREG might serve as a potential therapeutic target for fibrosis in CD.
Keywords: Effector CD4(+)T Cells; Inflammatory Bowel Diseases; Intestinal Inflammation; Intestinal Myofibroblasts.
Copyright © 2023 AGA Institute. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Fibrosis and Inflammation in Inflammatory Bowel Disease-More Than 2 Sides of the Same Coin?Gastroenterology. 2023 Jan;164(1):19-21. doi: 10.1053/j.gastro.2022.10.024. Epub 2022 Oct 29. Gastroenterology. 2023. PMID: 36341736 No abstract available.
References
-
- Cosnes J, Gower-Rousseau C, Seksik P, et al. Epidemiology and natural history of inflammatory bowel diseases. Gastroenterology 2011;140(6): 1785–94. - PubMed
-
- Rieder F, Fiocchi C. Intestinal fibrosis in inflammatory bowel disease – Current knowledge and future perspectives. J Crohns Colitis 2008;2(4): 279–90. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
