

Effects of different doses of methylprednisolone therapy on acute respiratory distress syndrome: results from animal and clinical studies
- PMID: 36114531
- PMCID: PMC9482269
- DOI: 10.1186/s12890-022-02148-y
Effects of different doses of methylprednisolone therapy on acute respiratory distress syndrome: results from animal and clinical studies
Abstract
Background: The optimal dose of glucocorticoids for acute respiratory distress syndrome (ARDS) is uncertain. This study aimed to evaluate the effects of different doses of methylprednisolone on sepsis-induced acute lung injury (ALI) rats and a cohort of moderate and severe ARDS patients.
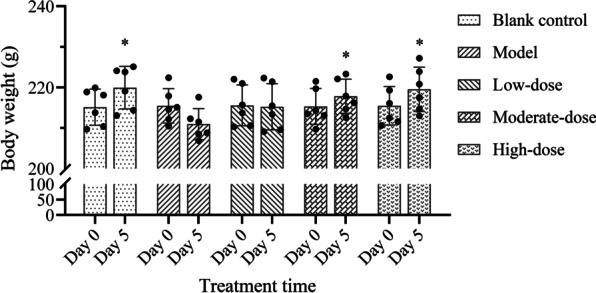
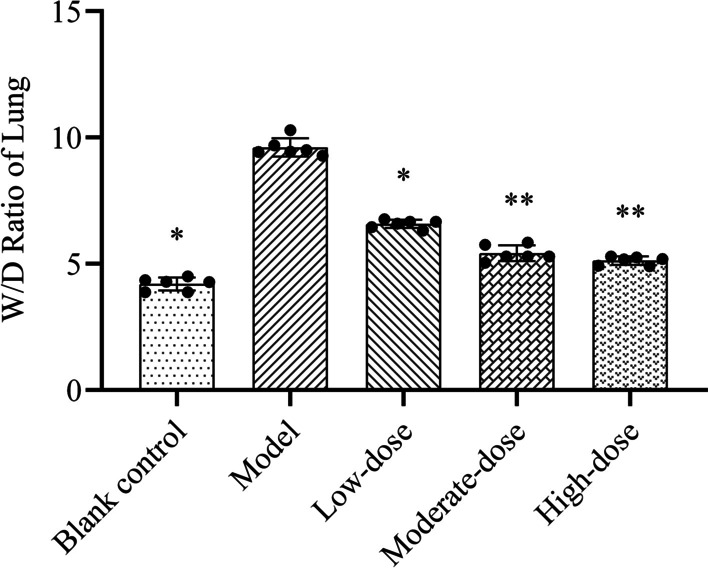
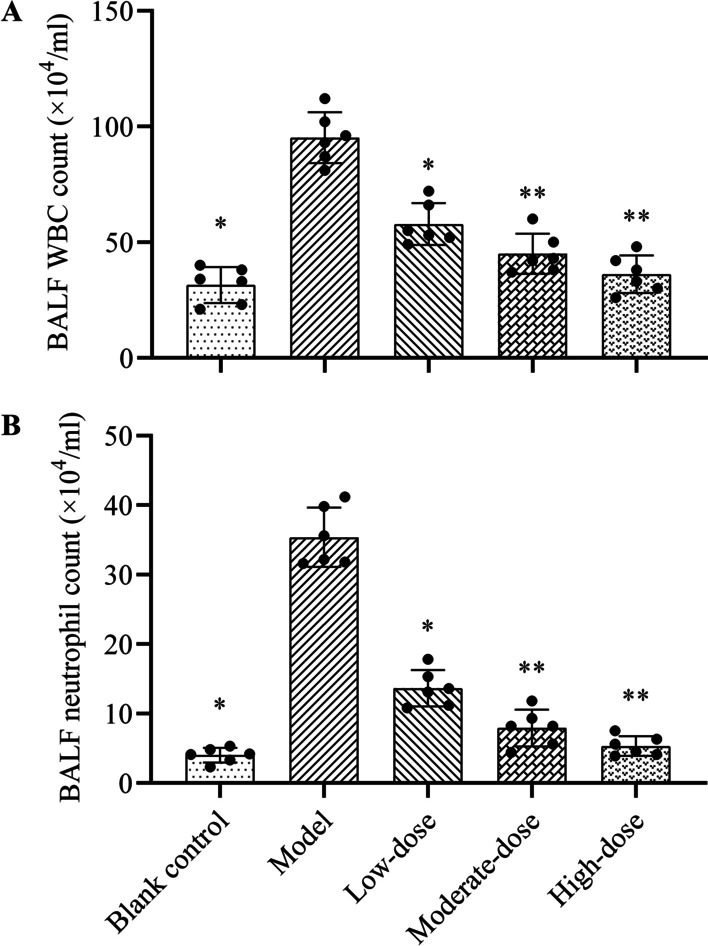
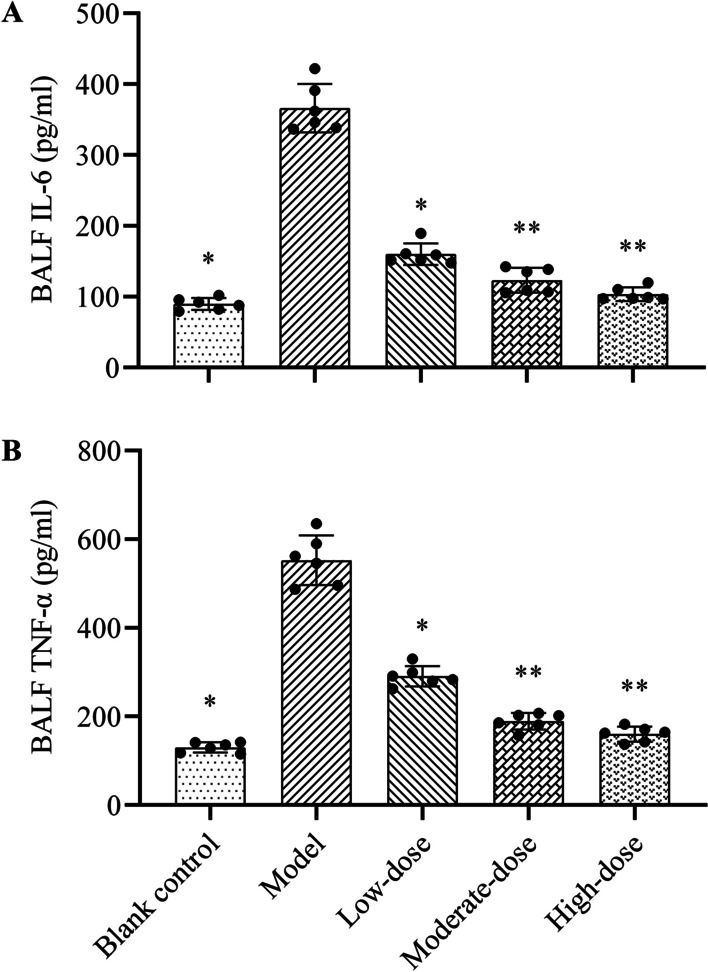
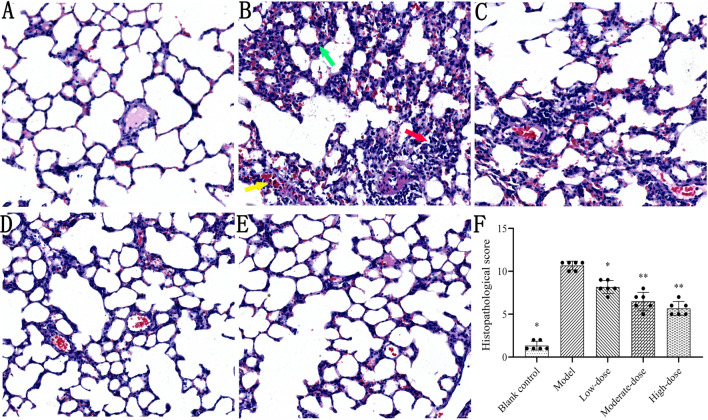
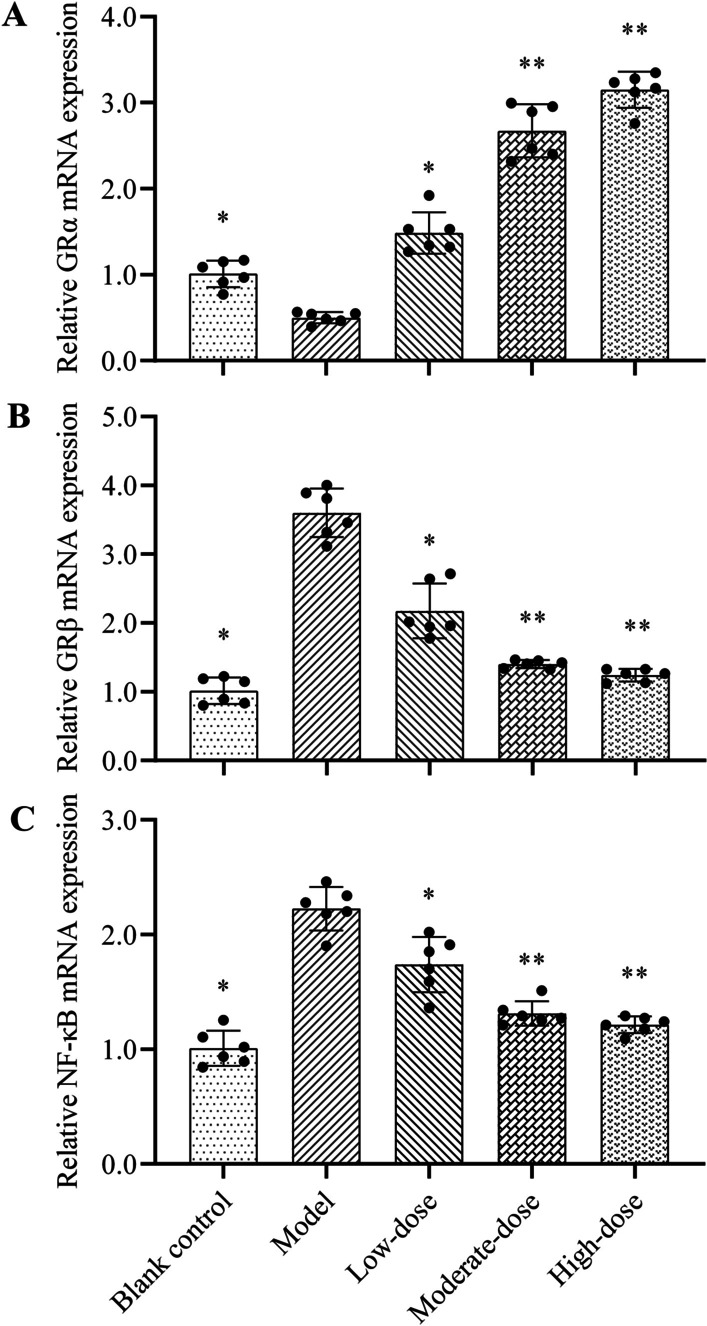
Methods: ALI rats, challenged with lipopolysaccharide, were randomly received intraperitoneal injection of normal saline (model group) and different doses of methylprednisolone (0.5, 2, 8 mg/kg, named as low-, moderate- and high-dose group, respectively) for 5 days. The body weight changes of rats, inflammatory factors in bronchoalveolar lavage fluid (BALF), lung wet/dry ratio, histopathological score, and the mRNA expressions of glucocorticoid receptor α (GRα), GRβ and nuclear factor-κB (NF-κB) were measured. Forty moderate and severe ARDS patients were treated with standard of care or plus different doses of methylprednisolone (40, 80, 120 mg/day, named as low-, moderate- and high-dose group, respectively) for 5 days. Clinical outcomes were PaO2/FiO2 ratio and C-reactive protein (CRP) level at day 5, intubation rate, hospital stay, 28-day mortality, and adverse events rate.
Results: In animal experiment, different doses of methylprednisolone could increase the body weight of rats, and reduce inflammatory factors in BALF and the degree of lung injury compared with model group. The efficacy of methylprednisolone at moderate-dose was better than that at low-dose, but was equivalent to that at high-dose, which was consistent with the differential changes in the mRNA expression of GRα, GRβ and NF-κB. In clinical study, the moderate-dose group was associated with higher PaO2/FiO2 ratio and lower CRP level. No significant difference in other clinical outcomes among groups was detected.
Conclusions: This study showed that the efficacy of methylprednisolone in ARDS treatment was not always dose-dependent due to the differential regulation of related receptors. The moderate-dose of methylprednisolone may be the potential optimal dose for ARDS treatment, which needs to be further verified by larger clinical trials.
Keywords: Acute lung injury; Acute respiratory distress syndrome; Animal model; Dose; Glucocorticoids; Methylprednisolone.
© 2022. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
[Comparative study of the protective effect of Xuebijing injection and Sivelestat sodium on acute lung injury/acute respiratory distress syndrome rats].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2022 Aug;34(8):837-841. doi: 10.3760/cma.j.cn121430-20220401-00334. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2022. PMID: 36177927 Chinese.
-
Effects of Zinc Finger Protein A20 on Lipopolysaccharide (LPS)-Induced Pulmonary Inflammation/Anti-Inflammatory Mediators in an Acute Lung Injury/Acute Respiratory Distress Syndrome Rat Model.Med Sci Monit. 2017 Jul 20;23:3536-3545. doi: 10.12659/msm.901700. Med Sci Monit. 2017. PMID: 28724884 Free PMC article.
-
Nuclear factor-kappaB- and glucocorticoid receptor alpha- mediated mechanisms in the regulation of systemic and pulmonary inflammation during sepsis and acute respiratory distress syndrome. Evidence for inflammation-induced target tissue resistance to glucocorticoids.Neuroimmunomodulation. 2005;12(6):321-38. doi: 10.1159/000091126. Neuroimmunomodulation. 2005. PMID: 16557033 Clinical Trial.
-
Efficacy and safety of methylprednisolone against acute respiratory distress syndrome: A systematic review and meta-analysis.Medicine (Baltimore). 2021 Apr 9;100(14):e25408. doi: 10.1097/MD.0000000000025408. Medicine (Baltimore). 2021. PMID: 33832136 Free PMC article.
-
Glucocorticoid Treatment in Acute Respiratory Distress Syndrome: An Overview on Mechanistic Insights and Clinical Benefit.Int J Mol Sci. 2023 Jul 28;24(15):12138. doi: 10.3390/ijms241512138. Int J Mol Sci. 2023. PMID: 37569514 Free PMC article. Review.
Cited by
-
Preliminary study on the protective effect of remazolam against sepsis-induced acute respiratory distress syndrome (ARDS).PeerJ. 2024 Apr 18;12:e17205. doi: 10.7717/peerj.17205. eCollection 2024. PeerJ. 2024. PMID: 38646480 Free PMC article.
-
Corticosteroids in ARDS.J Clin Med. 2023 May 8;12(9):3340. doi: 10.3390/jcm12093340. J Clin Med. 2023. PMID: 37176780 Free PMC article. Review.
-
The effect of budesonide delivered by high-frequency oscillatory ventilation on acute inflammatory response in severe lung injury in adult rabbits.Physiol Res. 2023 Dec 29;72(S5):S509-S521. doi: 10.33549/physiolres.935232. Physiol Res. 2023. PMID: 38165755 Free PMC article.
References
-
- Saguil A, Fargo MV. Acute respiratory distress syndrome: diagnosis and management. Am Fam Physician. 2020;101(12):730–738. - PubMed
-
- Critical Care Branch of Chinese Medical Association Guidelines for diagnosis and treatment of acute lung injury/acute respiratory distress syndrome (2006) Chin J Emerg Med. 2007;16(4):343–349.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
